Megaloblastic anemia is a hematological condition of low hemoglobin characterized by large, immature blood cells. These oversized cells are called megaloblasts, and the anemia they call megaloblastic anemia. It is a common condition and has an excellent prognosis if treated early.
What is Megaloblastic Anemia?
Anemia affects over 1.7 billion people worldwide. Megaloblastic anemia, also called macrocytic anemia, is a type of anemia. The name “Megaloblastic anemia” is derived from the Greek words “megaloblastic,” meaning large, immature cells, and “anemia,” meaning “without blood.”
The megaloblasts have large, spread-out nuclei.1Baldi, A., & Pasricha, S.-R. (2022). Anaemia: Worldwide Prevalence and Progress in Reduction. Springer EBooks, 3–17. https://doi.org/10.1007/978-3-031-14521-6_1
In addition to red blood cells, megaloblastic anemia involves changes in white blood cells. Large metamyelocytes are present, which is the name given to immature white blood cells.
Alongside the hallmark symptoms of anemia, such as fatigue and pallor, megaloblastic anemia causes neurological and cognitive issues. However, it is easily treatable if detected early.
How many people are affected by Megaloblastic Anemia?
Megaloblastic anemia is a common condition, affecting 2-4% of the world’s population. It affects both men and women, with distribution varying across countries. It is most common in vegetarians, elderly, and pregnant patients.2Moore, C. A., & Adil, A. (2022, July 11). Macrocytic Anemia. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK459295/
Causes of Megaloblastic Anemia
This is a result of impaired DNA production in the bone marrow. The bone marrow is the substance inside your bones. It is the site of the production of red blood cells. Since DNA synthesis is vital for the division and multiplication of cells, its impairment results in abnormal production of cells.3Anis Hariz, & Bhattacharya, P. T. (2023, April 3). Megaloblastic Anemia. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK537254/
There are a variety of causes of this abnormal DNA synthesis, such as:
Vitamin B12 Deficiency
Hypovitaminosis, or vitamin deficiency, the most common cause of this anemia. It results from deficiencies of vitamins B9 (folate) and B12. Both of these vitamins are vital for the normal production of DNA.
Vitamin B12 is found in food. It must attach to an intrinsic factor, a substance produced by the stomach and found in the small intestine. Vitamin B12 needs an intrinsic factor to be absorbed, and once inside the intestinal cells, the inherent factor gets moved. It then joins a protein carrier called transcobalamin II, which carries to the liver and other body tissues for use.
Once B12 has been absorbed into cells, it acts as a coenzyme in numerous reactions. It helps convert homocysteine into methionine, which is essential in the production of proteins. It also helps convert dihydrofolate to tetrahydrofolate, a necessary form of folic acid.
There are many causes of B12 deficiency, including but not limited to:
- Strict vegan diet
- Autoimmune conditions like pernicious anemia
- Inadequate absorption
- Chronic H. pylori infection
- Gastric surgery
- Gastritis
- Malignancies
- Nitrous oxide exposure4Green, R., & Miller, J. W. (2022). Vitamin B12 deficiency. Vitamins and Hormones, 405–439. https://doi.org/10.1016/bs.vh.2022.02.003
Vitamin B9 or Folate Deficiency
Vitamin B9, or folate, is also found in food. It is a part of giant molecules called polyglutamates, which your gut typically breaks down into monoglutamates and diglutamates. Your small intestine absorbs them and converts them into other forms: dihydrofolate, tetrahydrofolate, and methyl tetrahydrofolate, which circulates in the blood, enters cells and makes DNA with the assistance of B12.
There are several risk factors for folate deficiency:
- Gastric bypass surgery
- Malnutrition and reduced intake
- Certain medications
- Excessive alcohol
- Goat’s milk in infant’s diet
- Chronic hemolytic anemia5Khan, K. M., & Ishwarlal Jialal. (2023, June 26). Folic Acid Deficiency. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK535377/
Genetic Factors
Some hereditary disorders like thiamine-responsive megaloblastic anemia syndrome (TRMAS) cause a mutation in genes that regulate vitamin metabolism. Abnormal regulation affects DNA production. Other such disorders include:
- Methylmalonic acidemia with homocystinuria
- Homocystinuria due to cystathionine beta-synthase deficiency
- Hereditary orotic aciduria
- Lesch-Nyhan syndrome
Medicines & Drugs
Some medications and drugs can interfere with your DNA metabolism as well as vitamin absorption and cause megaloblastic anemia, such as:
- Acid reflux medication, e.g., proton pump inhibitors
- Anticancer drugs e.g. methotrexate, azathioprine
- Antiepileptic drugs, e.g., phenytoin
- Antiviral drugs, e.g., AIDS drugs like zidovudine
- Antibiotics, e.g., sulfonamides, trimethoprim
Dietary Choices
Not consuming a well-balanced diet leads to vitamin deficiencies, which cause megaloblastic anemia. There are several states in which the body does not get enough vitamin b9 and vitamin B12, for instance:
- Malnutrition
- Not consuming eggs and meat, which are rich sources of b12
- Not eating enough legumes, vegetables, and cereals, which are folate-dense foods
- Not eating enough nutrient-rich foods before and during pregnancy
Malabsorption
Malabsorption is the suboptimal absorption of nutrients in your gut. One such condition is pernicious anemia, in which the body cells attack cells in the stomach that produce a substance called the intrinsic factor. This intrinsic factor is necessary to absorb vitamin B12, and its deficiency causes megaloblastic anemia. Other malabsorption syndromes include:
- Celiac disease
- Crohn’s disease
- Chronic kidney disease
- Thyroid disorders
Pregnancy
There is an increased demand for nutrients during pregnancy. Because of factors such as improper diet or lack of supplementation, there can be vitamin deficiency in both the mother and fetus, leading to serious effects.
Old Age
Older adults have reduced gastric function as well as numerous chronic health conditions that require drugs, which reduce the absorption of vitamins in their gut. As a result, they are more likely to have megaloblastic anemia.6Green, R., & Ananya Datta Mitra. (2017). Megaloblastic Anemias. Medical Clinics of North America/the Medical Clinics of North America, 101(2), 297–317. https://doi.org/10.1016/j.mcna.2016.09.013
Symptoms of Megaloblastic Anemia
Following are some general and specific symptoms:
General Symptoms of Megaloblastic Anemia
Many symptoms of megaloblastic anemia are similar to those of other types of anemia, such as:
- Pale skin because of low blood flow
- Constantly feeling tired
- Feeling breathless at even slight exertion
- Palpitations and fast heartrate
- Changes in mood and irritability

Specific Symptoms of Megaloblastic Anemia
Other than general symptoms of anemia, there are various specific symptoms associated with the causes of megaloblastic anemia, especially B12 deficiency, such as:
- B12 is vital for the sound health of nerves. In its deficiency, peripheral nerves undergo damage. This damage results in neuropathic symptoms like:
o Tingling
o Numbness
o Pins and needles sensations - B12 deficiency also causes issues with cognition. It can make it hard to stay focused and function well. Sometimes, it even causes loss of memory and debilitating confusion. It can also cause speech impairment.
- B12 deficiency also causes loss of balance and abnormal gait.
- Other symptoms include:
o Jaundice
o Nausea
o Vomiting
How to diagnose megaloblastic anemia?
Megaloblastic anemia usually goes undiagnosed early on as it is mostly asymptomatic. So, it was discovered during a routine or incidental laboratory investigation. However, moderate and severe cases include several clinical findings from the physical examination.7Torrez, M., Chabot‐Richards, D., Babu, D., Lockhart, E., & Foucar, K. (2022). How I investigate acquired megaloblastic anemia. International Journal of Laboratory Hematology, 44(2), 236–247. https://doi.org/10.1111/ijlh.13789
History
Both anemia and vitamin deficiencies are marked by persistent, unresolved fatigue and tiredness. There may also be a few points in your history that would lead your physician to a megaloblastic anemia diagnosis:
- Being a vegetarian
- Being pregnant
- Having chronic health conditions
- Having autoimmune conditions like SLE, celiac disease
Physical Examination
Megaloblastic anemia presents asymptomatically at first. Later on, as the disease progresses, more and more symptoms become apparent. There are several physical findings associated with megaloblastic anemia, such as:
- Pallor
- Tiredness
- Brittle nails
- Neurological findings like numbness, loss of balance, and weakness
- Cognitive issues like memory loss and confusion
- Angular cheilitis (cracks at the corners of your mouth)
- Glossitis
- Enlarged liver and spleen
- Jaundice
- Heart failure (severe cases)
Lab Investigations
Megaloblastic anemia is diagnosed chiefly based on lab results depicting the following blood changes:8Boston Children’s Hospital. (2024). Childrenshospital.org. https://www.childrenshospital.org/conditions/megaloblastic-anemia
| Laboratory Finding | Description | Normal Range |
| Mean Corpuscular Volume | Increased to 110 to 115 fl | 77 to 93 fl |
| Mean Corpuscular Hemoglobin | Slightly increased | 27 to 32 pg |
| Mean Corpuscular Hemoglobin Concentration | Within normal limits | 20 to 25 g/dl |
| Hemoglobin | Typically low (may reach two g/dL) | ♀️12-16 g/dL ♂️13.5-17.5 d/dL |
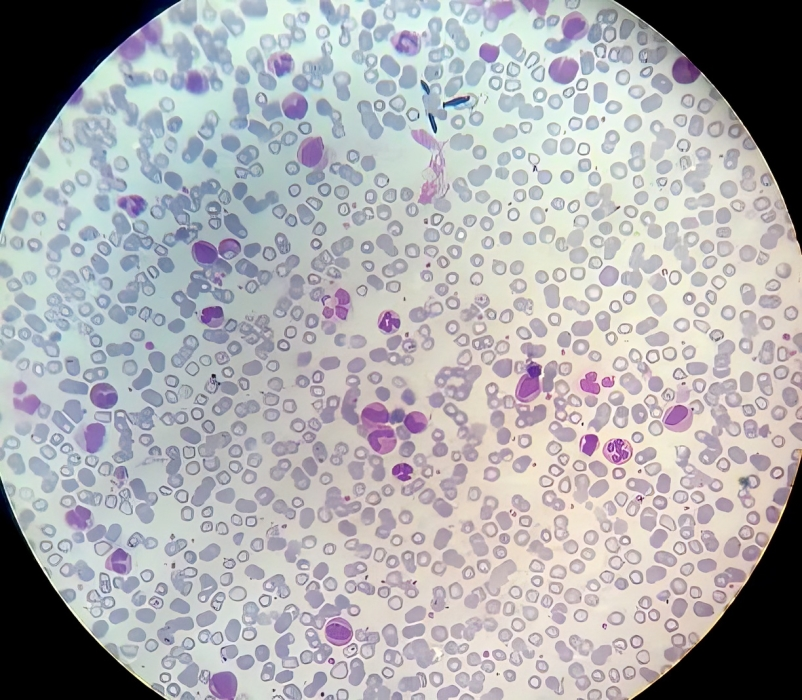
| Peripheral Blood Smear | Macrocytosis, hypersegmentation of neutrophils, anisocytosis, poikilocytosis, macroovalocytes | |
| Differential Leukocyte Count | Marked neutropenia, relative lymphocytosis |
How can Megaloblastic Anemia caused by B12 deficiency be treated?
Medications, including supplements, injections, and dietary changes, are the go-to treatment for B12 deficiency-related megaloblastic anemia.
Medications
The medications mainly include preparations of B12 in intramuscular or subcutaneous injection and oral form. Nasal sprays of B12 are usually avoided.9 UpToDate. (2024). Uptodate.com. https://www.uptodate.com/contents/treatment-of-vitamin-b12-and-folate-deficiencies
| Condition | Initial Dose | Maintenance Dose | Route |
| Due to permanently impaired absorption, e.g., in pernicious anemia | 1000 mcg daily | 100-1000 mcg monthly | Intramuscular/
Subcutaneous |
| Due to poor nutrition | 25-2000 | – | Oral |
B12 Injections
B12 Injections are used in patients whose B12 deficiency is caused by pernicious anemia and other similar conditions. You usually have to take them for life if you do not have normal intestinal absorption of B12.
Initially, 1000 mcg is administered daily through intramuscular or subcutaneous injection. This continues for a week. Afterward, you will get a monthly maintenance dose of 100-1000 mcg.
Oral B12 Supplements
The usual dose for adults with B12 deficiency is 25 to 2000 mcg, given orally daily. Children are given 0.5 to 3 mcg every day.
Dietary Modification
Dietary changes can resolve mild to moderate nutritional B12 deficiency without any medications. These include taking more:
- Red meat, especially liver
- Poultry
- Fish
- Eggs
- Milk and dairy products
- B12- fortified foods
o Cereals
o Plant-based milk alternatives
Lifestyle Changes
You can adopt certain habits and avoid others to resolve your B12 deficiency:
- Limit alcohol
- Manage chronic diseases
- Discuss alternative medicines if drugs are causing your B12 deficiency
How is Megaloblastic Anemia caused by Folate deficiency treated?
Megaloblastic anemia caused by folate deficiency is treated using various medications and nutritional modifications.
Medications
Folate deficiency is treated using folate tablets and B12 supplements.10Coffey-Vega, K. (2023, June 30). Folate Deficiency Treatment & Management: Approach Considerations, Prevention. Medscape.com; Medscape. https://emedicine.medscape.com/article/200184-treatment
| Clinical Circumstance | Dosage | Duration |
| Poor dietary intake or drugs | 5 mg/day | Four months |
| Malabsorption | Up to 15 mg/day | Four months |
| Prophylaxis for chronic hemolytic states and kidney dialysis | 5 mg daily to weekly |
Sometimes, folate deficiency results from B12 deficiency. If you have both deficiencies, you will be given B12 supplementation as well.
Dietary Modification
Your healthcare provider will counsel you on foods rich in folate. Some of them are:
- Eggs
- Liver
- Leafy green vegetables
- Legumes
- Lentils
- Nuts
- Fortified cereals
Lifestyle Changes
Like B12 deficiency, folate deficiency can be resolved by cutting down on excess alcohol and managing your nutrition well if you have any health conditions.
How to prevent Megaloblastic Anemia?
The best approach to prevent megaloblastic anemia is to ensure adequate stores of vitamins B12 and folate in the body. For this, a person should consume enough vitamins through diet and supplements, and their body should absorb enough of them. Doctors should also counsel patients about different health conditions, drugs, lifestyles, and their effect on nutrient absorption. The requirements for the vitamins are as follows:11Office of Dietary Supplements – Vitamin B12. (2017). Nih.gov. https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
| Population | Vitamin B12 Requirement (mcg/day) | Folate Requirement (mcg/day) |
| Birth to 6 months | 0.4 | 65 |
| Children and adolescents (14 to 18 years) | 2.4 | 400 |
| Adults | 2.4 | 400 |
| Pregnancy | 2.6 | 600 |
| Lactation | 2.8 | 500 |
Prognosis of Megaloblastic Anemia
Megaloblastic anemia has an excellent prognosis. Patients make a full recovery. Mild to moderate disease resulting from poor nutrition usually resolves with lifestyle and dietary changes.
However, causes must be addressed early and treated promptly. They can have devastating effects if they go undetected, e.g., folate deficiency in pregnant patients, causing neural tube defects in the fetus. These are debilitating developmental disorders of the spinal cord that are easily preventable with prophylaxis.12Safi, J., L. Joyeux, & Chalouhi, G. E. (2012). Periconceptional Folate Deficiency and Implications in Neural Tube Defects. Journal of Pregnancy, 2012, 1–9. https://doi.org/10.1155/2012/295083
Megaloblastic Anemia vs. Pernicious Anemia
Megaloblastic anemia is an anemia with large-sized immature red blood cells in the body. Pernicious anemia is a particular type of megaloblastic anemia accompanied by an autoimmune disorder that destroys the production of intrinsic factors in the body, resulting in lifelong B12 deficiency.
Microcytic Anemia vs Megaloblastic Anemia
In microcytic anemia, red blood cells become smaller than their regular size, e.g., iron deficiency anemia, thalassemia, and anemia of chronic disease. In megaloblastic anemia, your bone marrow produces many large-sized, underdeveloped red blood cells, as seen in B12 and folate deficiencies.
Conclusion
Megaloblastic anemia is a type of anemia that causes red blood cells to become immature and larger than usual. It is usually caused by a lack of intake or poor absorption of vitamins B12 and folate. Megaloblastic anemia has a good prognosis and can be fully managed with supplements, better nutrition, and lifestyle changes.
Refrences
- 1Baldi, A., & Pasricha, S.-R. (2022). Anaemia: Worldwide Prevalence and Progress in Reduction. Springer EBooks, 3–17. https://doi.org/10.1007/978-3-031-14521-6_1
- 2Moore, C. A., & Adil, A. (2022, July 11). Macrocytic Anemia. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK459295/
- 3Anis Hariz, & Bhattacharya, P. T. (2023, April 3). Megaloblastic Anemia. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK537254/
- 4Green, R., & Miller, J. W. (2022). Vitamin B12 deficiency. Vitamins and Hormones, 405–439. https://doi.org/10.1016/bs.vh.2022.02.003
- 5Khan, K. M., & Ishwarlal Jialal. (2023, June 26). Folic Acid Deficiency. Nih.gov; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK535377/
- 6Green, R., & Ananya Datta Mitra. (2017). Megaloblastic Anemias. Medical Clinics of North America/the Medical Clinics of North America, 101(2), 297–317. https://doi.org/10.1016/j.mcna.2016.09.013
- 7Torrez, M., Chabot‐Richards, D., Babu, D., Lockhart, E., & Foucar, K. (2022). How I investigate acquired megaloblastic anemia. International Journal of Laboratory Hematology, 44(2), 236–247. https://doi.org/10.1111/ijlh.13789
- 8Boston Children’s Hospital. (2024). Childrenshospital.org. https://www.childrenshospital.org/conditions/megaloblastic-anemia
- 9UpToDate. (2024). Uptodate.com. https://www.uptodate.com/contents/treatment-of-vitamin-b12-and-folate-deficiencies
- 10Coffey-Vega, K. (2023, June 30). Folate Deficiency Treatment & Management: Approach Considerations, Prevention. Medscape.com; Medscape. https://emedicine.medscape.com/article/200184-treatment
- 11Office of Dietary Supplements – Vitamin B12. (2017). Nih.gov. https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
- 12Safi, J., L. Joyeux, & Chalouhi, G. E. (2012). Periconceptional Folate Deficiency and Implications in Neural Tube Defects. Journal of Pregnancy, 2012, 1–9. https://doi.org/10.1155/2012/295083
