Androgenic Alopecia (AGA), also referred to as ‘androgenetic alopecia’, is a common, progressive, non-scarring type of hair loss condition that arises due to miniaturization of scalp hair follicles as they become more sensitive to dihydrotestosterone. Also called male pattern baldness or female pattern baldness, it affects approximately 50% of men and 30% of women by the age of 50.1Ho CH, Sood T, Zito PM. Androgenetic Alopecia. [Updated 2024 Jan 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430924/
Androgenic alopecia (AGA) is widely recognized as a potential marker for cardiovascular diseases in men and polycystic ovarian syndrome in women.2Qureshi, H. F., Akhtar, A., Kakar, A., Sakina, S., Irum, S., & Nasr, N. (2024). Association of Androgenetic Alopecia with Metabolic Syndrome. Journal of the College of Physicians and Surgeons–Pakistan: JCPSP, 34(10), 1245–1248. https://doi.org/10.29271/jcpsp.2024.10.1245
Owing to its psychosocial implications, it’s essential to know the stages, diagnostic approach, and treatment options to manage it effectively.
How common is Androgenic Alopecia?
It is extremely common and increases with age. One study reported that around 50% of men experience AGA by age 50, increasing to 80% by age 70.3He, H., Xie, B., & Xie, L. (2018). Male pattern baldness and incidence of prostate cancer: A systematic review and meta-analysis. Medicine, 97(28), e11379. https://doi.org/10.1097/MD.0000000000011379
Women get AGA too, but it’s less common than in men. One study from Brazil found that about 32% of adult women had AGA, which rises to about 68% by the age of 75.4Ramos, P. M., Melo, D. F., Radwanski, H., & Miot, H. A. (2023). Female-pattern hair loss: Therapeutic update. Anais Brasileiros de Dermatologia, 98(4), 506. https://doi.org/10.1016/j.abd.2022.09.006
What causes Androgenic Alopecia?
An interplay of hormonal, genetic, and metabolic factors causes androgenic alopecia:
Genetic Causes:
Specific genetic markers on the androgen receptor (AR) gene, also called rs6152, are linked to an increased risk of AGA. This gene marker increases the chances of developing AGA by threefold. 5Zhuo, F. L., Xu, W., Wang, L., Wu, Y., Xu, Z. L., & Zhao, J. Y. (2012). Androgen receptor gene polymorphisms and risk for androgenetic alopecia: a meta-analysis. Clinical and experimental dermatology, 37(2), 104–111. https://doi.org/10.1111/j.1365-2230.2011.04186.x
Additionally, scientists also link the GGN repeat with hair loss. The GGN repeat is a short DNA code pattern that may change the androgen receptor activity. This change can raise the risk of early baldness by around 46%. Several other genes (AR, EDA2R, SRD5A2, etc.) also contribute to how hair follicles respond to DHT. 6Hillmer, A. M., Hanneken, S., Ritzmann, S., Becker, T., Freudenberg, J., Brockschmidt, F. F., Flaquer, A., Freudenberg-Hua, Y., Jamra, R. A., Metzen, C., Heyn, U., Schweiger, N., Betz, R. C., Blaumeiser, B., Hampe, J., Schreiber, S., Schulze, T. G., Hennies, H. C., Schumacher, J., . . . Nöthen, M. M. (2005). Genetic Variation in the Human Androgen Receptor Gene Is the Major Determinant of Common Early-Onset Androgenetic Alopecia. American Journal of Human Genetics, 77(1), 140. https://doi.org/10.1086/431425
Hormonal Causes:
Our hair follicles have an enzyme called 5-alpha reductase that converts the male sex hormone Testosterone into a more potent form called dihydrotestosterone (DHT). DHT then impacts hair follicles in people who are genetically sensitive to it in the following way:
- DHT attaches to the androgen receptor on the hair follicle.
- This attachment sends a signal to the hair follicle to shrink, a process known as miniaturization.
- Over time, the hair becomes thinner, shorter, and weaker.
- In advanced stages, the follicle may stop producing visible terminal hairs. 7Cuevas-Diaz Duran, R., Martinez-Ledesma, E., Garcia-Garcia, M., Gauzin, D. B., Sarro-Ramírez, A., Gonzalez-Carrillo, C., Rodríguez-Sardin, D., Fuentes, A., & Cardenas-Lopez, A. (2024). The Biology and Genomics of Human Hair Follicles: A Focus on Androgenetic Alopecia. International Journal of Molecular Sciences, 25(5), 2542. https://doi.org/10.3390/ijms25052542
Environmental Causes:
If you carry the genes for AGA, your environment and your lifestyle choices can influence how quickly and how severely those genes become active.
- According to a study on identical twins (those who share the same genetics), the twin with higher stress levels, smoking habits, dandruff, alcohol use, and a poor diet experienced more severe hair loss as compared to the other. So, even if two people have similar genetic makeup, your lifestyle, stress levels, dietary intake, and habits render a big difference in how quickly you’ll experience hair loss.8Gatherwright, J., Liu, M. T., Amirlak, B., Gliniak, C., Totonchi, A., & Guyuron, B. (2013). The contribution of endogenous and exogenous factors to male alopecia: a study of identical twins. Plastic and reconstructive surgery, 131(5), 794e801e. https://doi.org/10.1097/PRS.0b013e3182865ca9
- Also, scientists recently discovered that certain gut bacteria influence the development of AGA. It is a brand new area of research and awaits conclusive evidence. 9Liu, J., Luo, W., Hu, Z., Zhu, X., & Zhu, L. (2024). The causal relationship between gut microbiota and androgenetic alopecia: A Mendelian randomization study. Medicine, 103(52), e41106. https://doi.org/10.1097/MD.0000000000041106
Symptoms of Androgenic Alopecia
Androgenic alopecia is characterized by progressive thinning of scalp hair, exhibiting a distinct pattern.
Gradual Hair Thinning:
AGA starts gradually and progresses slowly in the specific regions of the scalp.
- In men, the hairline recedes at the temple first, forming an “M” shape, followed by thinning at the crown. With time, these areas of baldness expand and merge.
- In women, there is diffuse thinning across the scalp. The frontal hairline usually remains intact.
Increased Hair Shedding:
You might notice more hair falling out, especially while combing, brushing, or washing. In contrast to physiological hair loss, this shedding is more frequent and follows a noticeable pattern.
Miniaturization of Hair:
Progressively, your hair follicles shrink, making your hair thinner and weaker. This phenomenon is called miniaturization and is considered a hallmark of androgenic alopecia.
Scalp Appearance:
Since it’s a non-scarring condition, you won’t notice any itching, burning, inflammation, or pain. The scalp in AGA remains smooth and intact, with hair follicles still present, though miniaturized.
Psychological Effects:
Not everyone feels affected by hair loss. But for many, androgenic alopecia can impact confidence, self-esteem, and emotional well-being. Seeing your hair thin out, especially when you’re still young, can really affect your confidence and cause stress or anxiety.
Stages of Androgenic Alopecia
Understanding the stages of androgenic alopecia isn’t just about knowing how hair loss progresses. It plays an instrumental role in the diagnosis, treatment, and patient communication.
Stages of Male Androgenic Alopecia:
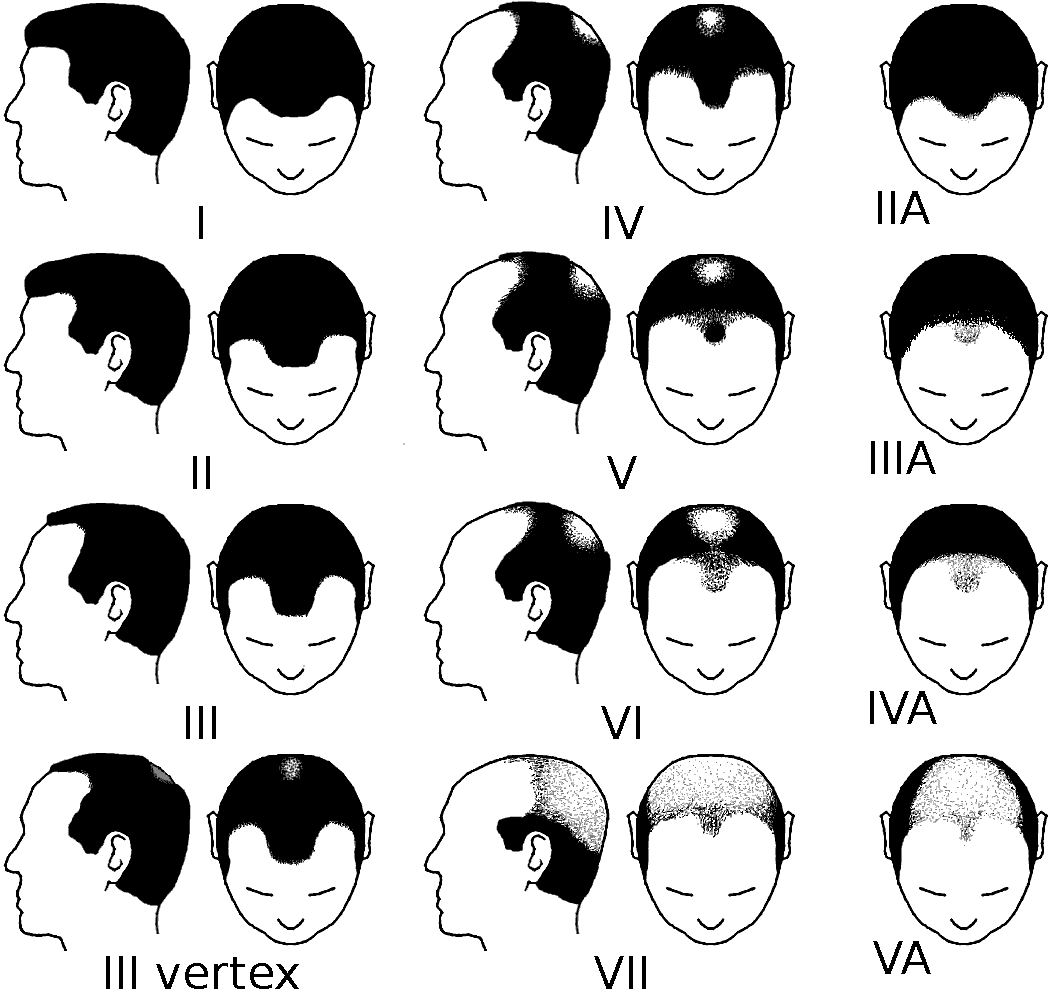
The Hamilton-Norwood scale is a standard to classify male androgenic alopecia. This scale identifies the seven stages (I-VII) with minimal recession (stage I) to extensive vertex and frontal hair shedding (stage VII). These stages are:10Henne, S. K., & Heilmann-Heimbach, S. (2023). Male-pattern hair loss: Comprehensive identification of the associated genes as a basis for understanding pathophysiology. Medizinische Genetik, 35(1), 3. https://doi.org/10.1515/medgen-2023-2003
- Stage I: This is a baseline stage, characterized by no visible hair loss or only mild recession of the hairline.
- Stage II: It involves a slight recession at the temple forming an “M” shaped hairline. There is no thinning of hair at the crown. This stage signals the beginning of androgen-sensitive miniaturization in genetically prone individuals.
- Stage III: It is the earliest stage that involves clinically visible recession. In this stage, the hairline moves back evenly at the temples, usually more than 2 cm from the original hairline.
- Stage IV: In this stage, the hair loss is severe at both the frontal and vertex regions. But a band of hair still separates the two bald areas.
- Stage V: The bridge of hair becomes thinner as hair shedding further increases at the frontal and crown areas. As the balding areas come closer, the scalp starts to look more exposed.
- Stage VI: No visible separation between your frontal and vertex bald areas in this stage.
- Stage VII: It is the most advanced stage with extensive hair loss on the top of the scalp. Only a narrow rim of hair remains along the sides and back.
Stages of Female Androgenic Alopecia:
Ludwig’s scale classifies female androgenic alopecia into the following three stages:11Bhat, Y. J., Latif, I., & Hassan, I. (2020). Female Pattern Hair Loss—An Update. Indian Dermatology Online Journal, 11(4), 493.
- Grade I: Mild thinning of hair across the crown
- Grade II: More noticeable hair thinning, causing the scalp to become more visible.
- Grade III: Extensive thinning, making the scalp at the crown visible.

How is Androgenic Alopecia diagnosed?
Androgenic alopecia is mainly diagnosed through a clinical examination. The doctor may use additional methods to rule out other types of hair loss.
Clinical History:
Diagnosing AGA starts with a detailed medical history. Your doctor may ask you about the onset, progression, and family background of hair loss. The characteristic pattern of AGA is the diagnostic clue.
Physical Examination:
Hair Pull Test
The hair pull test is a simple method used to check for active hair shedding. In this test, your doctor gently pulls about 50–60 hairs from your scalp.
The hair pull test in AGA is typically negative, meaning fewer than 6 hairs are extracted per pull.
Trichoscopy
It is a non-invasive, magnified scalp examination. In AGA, trichoscopy typically shows the following findings:
- Hair diameter variability – You’ll notice a mix of thick and thin hairs on the scalp.
- Vellus hairs – Fine, short hairs become more common as AGA progresses.
- Peripilar sign – A brownish halo often appears around hair follicle openings.
These features help your dermatologist to distinguish AGA from other conditions. Trichoscopy also helps in the monitoring of treatment response over time.
Scalp Biopsy:
A scalp biopsy is not usually needed in AGA. Your doctor might recommend it if the cause of your hair loss is uncertain or doesn’t follow a typical pattern. A biopsy sample of AGA often shows:
- Lack of inflammation.
- Increased miniaturized follicles.
- Shift in the usual hair growth cycle, with fewer hairs in the growing phase and more entering the shedding phase.
Laboratory Tests:
Blood tests are not usually needed for AGA, except when suspecting other underlying medical conditions, like thyroid disease or iron deficiency. These tests may include:
- Dehydroepiandrosterone Sulfate (DHEAS)
- Serum testosterone
- Thyroid Function
- Ferritin levels
- Iron levels
Other labs may include:
- Cardiovascular evaluation to screen for concurrent CVS abnormalities in men
- Hormonal profile to rule out PCOS in women
Differential Diagnosis
AGA must be differentiated from other hair loss conditions:
- Telogen Effluvium: It causes sudden, diffuse hair shedding. Unlike AGA, the hair pull test is usually positive in telogen effluvium.
- Cicatricial Alopecia: It refers to a group of scarring hair loss disorders. Hair follicles are permanently damaged in these conditions, manifesting as redness, scaling, and loss of follicular openings, unlike the smooth scalp in AGA.
- Alopecia Areata (AA): It is an autoimmune disorder that causes sudden patchy hair loss with a smooth, non-scarring scalp. Hair loss pattern is irregular, and regrowth is usually possible. In contrast to AGA, it involves no gradual thinning or frontal recession.
- Traction Alopecia: It’s a mechanical hair loss caused by chronic pulling from tight hairstyles, especially around the hairline.
- Trichotillomania: It’s a psychiatric condition in which individuals compulsively pull out their own hair, resulting in irregular patches. Unlike AGA, trichotillomania is often accompanied by psychological stress or anxiety disorders.
- Thyroid or Nutritional Hair Loss: Hair loss due to hypothyroidism or deficiency of iron and vitamin D can mimic AGA. These conditions generally cause diffuse thinning without a specific pattern and may improve with respective treatments.
Trichoscopy is especially useful in distinguishing these disorders and in preventing unnecessary biopsies.
Androgenic Alopecia Vs. Alopecia Areata:
Although both cause hair loss, androgenic alopecia and alopecia areata differ significantly in their patterns, causes, and progression.
| Feature | Androgenic Alopecia (AGA) | Alopecia Areata (AA) |
| Type of Hair Loss | Gradual, patterned thinning | Sudden, patchy hair loss |
| Onset | Slowly over the years | Often rapid, within days or weeks |
| Pattern | Men: receding hairline & crown Women: crown thinning | Sudden onset with circular or irregular patches anywhere on the scalp |
| Hair Pull Test | Usually negative | Often positive in active patches |
| Miniaturization | Yes. Thick hairs become thin and short | No. Sudden hair loss without miniaturization |
| Regrowth | Slow and incomplete without treatment | Often regrows spontaneously or with treatment |
| Cause | Genetic + hormonal (DHT sensitivity) | Autoimmune, the body attacks its own hair follicles |
| Age Group | Common after puberty, worsens with age | It can occur at any age, even in children |
| Treatment | Minoxidil, finasteride, hair transplant | Steroids, topical immunotherapy, JAK inhibitors |
Treatment options for Androgenic Alopecia
There are several treatment options for androgenic alopecia, ranging from topical and oral medications to advanced therapies like PRP, lasers, and hair transplantation.
Topical Minoxidil:
Minoxidil is a vasodilator that increases blood flow to the scalp. It is a first-line treatment for AGA for both men and women. It slows down the progression and helps to regrow hair by prolonging the anagen or growth phase of the hair cycle.
Its typical side effects include scalp irritation and a transient increase in shedding initially. These side effects are usually manageable and tend to settle with continued use.12Kaliyadan, F. (2022). Androgenetic alopecia – medical management. Clinical Dermatology Review, 6(2), 75–79. https://doi.org/10.4103/cdr.cdr_27_21
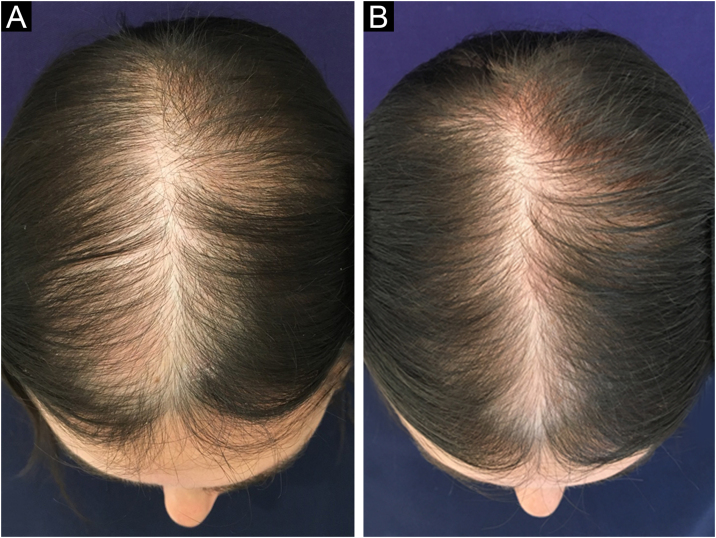
Image adapted from: Female pattern hair loss: therapeutic update. Available from: https://www.researchgate.net/figure/Clinical-improvement-in-a-patient-with-FPHL-using-minoxidil-5-solution-1-a-day-A_fig1_369673893 [Accessed 7 Jul 2025]. Licensed under CC BY 4.0.
Topical Finasteride:
Lower doses (0.25%) of topical finasteride are a safer option for both men and women, which minimizes the systemic side effects of finasteride. Using topical finasteride with minoxidil gives significantly better results than using minoxidil alone.13Asad, N., Naseer, M., & Ghafoor, R. (2024). Efficacy of Topical Finasteride 0.25% With Minoxidil 5% Versus Topical Minoxidil 5% Alone in Treatment of Male Pattern Androgenic Alopecia. Journal of drugs in dermatology: JDD, 23(11), 1003–1008.
Oral Finasteride:
It is the only FDA-approved systemic option for AGA in men. Oral finasteride slows down follicle miniaturization and supports hair regrowth by blocking the 5-alpha reductase enzyme.
Side effects of oral finasteride may include decreased libido, erectile dysfunction, and gynecomastia.
Low-Level Laser Therapy (LLLT):
LLLT is a non-invasive device-based option in which your doctor asks you to use specialized combs, helmets, and caps that emit red or infrared lights.
Some studies have shown that LLLT can noticeably improve hair density in both men and women. But it’s still considered experimental. Doctors need more studies before they can confidently recommend it as a go-to treatment.14Liu, K. H., Liu, D., Chen, Y. T., & Chin, S. Y. (2019). Comparative effectiveness of low-level laser therapy for adult androgenic alopecia: a systematic review and meta-analysis of randomized controlled trials. Lasers in medical science, 34(6), 1063–1069. https://doi.org/10.1007/s10103-019-02723-6
Platelet Rich Plasma (PRP):
PRP uses concentrated growth factors from your own blood. These are injected into your scalp to boost hair growth naturally.
Current evidence suggests that PRP can moderately improve hair density and thickness, especially in early-stage androgenic alopecia. However, results may vary, and it is not yet considered a first-line treatment.
Hair Transplantation:
If medical treatments don’t help, hair transplant surgery can be a more long-lasting option. Hair transplantation involves:
- Follicular Unit Transplantation (FUT): Also known as the strip method, this technique involves removing a strip of scalp from the back of the head, separating it into small follicular units, and transplanting them into balding areas.
- Follicular Unit Extraction (FUE): It involves extracting individual hair follicles one by one from the scalp and placing them into areas with visible thinning or bald patches.
Addressing the Psychological Stress:
Hair fall is often a stressful event for many. This stress further worsens hair loss. Therefore, it is important to address the psychological and emotional toll that comes with AGA. Some of the stress management techniques that can help patients cope better with stress are:
- Supportive Psychotherapy
- Cognitive Behavioral Therapy (CBT)
- Joining relevant support groups
Patient Counselling & Follow-up:
The significance of patient counseling and follow-ups can’t be overemphasized:
- Counsel your patients about the course of treatment and set realistic expectations
- Educate them that, within three months, they might notice some reduction in hair fall. By six months, they might observe visible improvement in hair density and coverage, and the maximum expected benefit might be achieved by one year.
- Patients should also be counseled about the role of patient compliance in the prognosis of this condition.
- Also, encourage your patients to check in at 3, 6, and 12 months, bringing their treatment logbooks to help boost motivation and track outcomes effectively.
Diet for Androgenic Alopecia
While AGA is primarily genetic and hormonal, there are certain foods that may aggravate or alleviate it.
Foods that may aggravate AGA :
These include:
- Excess dairy: It can cause a hormonal imbalance, particularly in PCOS patients.
- Foods with a high glycemic index, such as white bread and artificial sugar, increase insulin and IGF-1 levels, leading to increased androgen production.
- Scientists also associate ultra-processed foods with oxidative stress and chronic inflammation, contributing further to hair loss.15Bazmi, S., Sepehrinia, M., Pourmontaseri, H., Bazyar, H., Vahid, F., Farjam, M., Dehghan, A., Hébert, J. R., Homayounfar, R., & Shakouri, N. (2024). Androgenic alopecia is associated with a higher dietary inflammatory index and a lower antioxidant index score. Frontiers in Nutrition, 11, 1433962.
Better to avoid these to have a healthier scalp environment.
Foods that alleviate AGA:
These include:
- Foods containing nutrients important for overall hair health, such as Vitamin B-complex, Vitamin D, Vitamin A, Vitamin C, Iron, Zinc, Selenium, Manganese, and Copper. Deficiencies of these nutrients can disrupt the normal hair cycle and contribute to the progression of androgenic alopecia.
- Food items that inhibit the 5-alpha reductase enzyme. For example, saw palmetto supplements, pumpkin seed oil, Epigallocatechin gallate (EGCG) green tea, and reishi mushrooms
Practical Guidelines:
- Avoid crash diets as they are notorious for aggravating hair loss
- Consume a diet rich in healthy fats, fruits, vegetables, lean proteins, and whole foods
- If you have an underlying medical disorder such as PCOS or insulin resistance, consult a dietitian.
- And yes, continue your medical treatment side-by-side as these measures only serve as an adjunct, not a replacement for what your doctor advises.
Can I prevent Androgenic Alopecia?
Since androgenic alopecia is largely genetic, complete prevention isn’t always possible. Early intervention is more effective than treating late-stage AGA.
Early Treatment:
If you have a strong family history of early AGA, it’s better to start treatment as early as possible. Using topical minoxidil or finasteride may help delay follicle shrinkage and slow down hair loss.
Healthy Lifestyle:
By staying active, eating right, and keeping your weight in check, you can always slow down the progression of Androgenic alopecia:
- Poor sleep triggers inflammation in the body, disturbing the hair growth cycle. Getting better sleep may help slow down hair loss.
- Chronic stress raises cortisol levels, and this speeds up hair fall. That’s why managing stress is important for your hair, too.
- Quitting smoking also improves scalp health by restoring healthy blood flow to your hair follicles.
Hair Care:
Hair care doesn’t stop the progression of AGA. It helps minimize any compounding damage, making your scalp healthier and more receptive to medical treatment.
- Avoid tight hairstyles, heat styling, and harsh shampoos.
- Use mild, sulfate-free shampoos and massage your scalp regularly to boost circulation.
- Wear a hat outdoors or use UV-protectant sprays to minimize scalp sun damage.
Prognosis of Androgenic Alopecia
Androgenic alopecia is not a life-threatening condition. It may linger for a while, but it’s manageable, with a good prognosis. Positive prognostic factors include:
- Timely diagnosis and early treatment
- Absence of other comorbidities, such as cardiovascular disease or PCOS
- Patient compliance with treatment
- Mild to moderate miniaturization
With treatment adherence, hair loss stabilizes in the majority of patients. Some even have hair regrowth, especially if they had started treatment early, and stick to their doctor’s advice.
Conclusion
Androgenic alopecia is one of the most common types of hair loss. While its causes are mainly genetic and hormonal, lifestyle and diet also play key roles in how early and how fast it progresses. Understanding the symptoms and getting a proper diagnosis early can help you take timely action. Today, there are many effective androgenic alopecia treatment options, from minoxidil and finasteride to PRP and hair transplants. Even changes in your diet, stress levels, and sleep can make a difference. Stay informed, act early, and talk to your doctor to choose a plan that fits your stage and personal needs.
Refrences
- 1Ho CH, Sood T, Zito PM. Androgenetic Alopecia. [Updated 2024 Jan 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430924/
- 2Qureshi, H. F., Akhtar, A., Kakar, A., Sakina, S., Irum, S., & Nasr, N. (2024). Association of Androgenetic Alopecia with Metabolic Syndrome. Journal of the College of Physicians and Surgeons–Pakistan: JCPSP, 34(10), 1245–1248. https://doi.org/10.29271/jcpsp.2024.10.1245
- 3He, H., Xie, B., & Xie, L. (2018). Male pattern baldness and incidence of prostate cancer: A systematic review and meta-analysis. Medicine, 97(28), e11379. https://doi.org/10.1097/MD.0000000000011379
- 4Ramos, P. M., Melo, D. F., Radwanski, H., & Miot, H. A. (2023). Female-pattern hair loss: Therapeutic update. Anais Brasileiros de Dermatologia, 98(4), 506. https://doi.org/10.1016/j.abd.2022.09.006
- 5Zhuo, F. L., Xu, W., Wang, L., Wu, Y., Xu, Z. L., & Zhao, J. Y. (2012). Androgen receptor gene polymorphisms and risk for androgenetic alopecia: a meta-analysis. Clinical and experimental dermatology, 37(2), 104–111. https://doi.org/10.1111/j.1365-2230.2011.04186.x
- 6Hillmer, A. M., Hanneken, S., Ritzmann, S., Becker, T., Freudenberg, J., Brockschmidt, F. F., Flaquer, A., Freudenberg-Hua, Y., Jamra, R. A., Metzen, C., Heyn, U., Schweiger, N., Betz, R. C., Blaumeiser, B., Hampe, J., Schreiber, S., Schulze, T. G., Hennies, H. C., Schumacher, J., . . . Nöthen, M. M. (2005). Genetic Variation in the Human Androgen Receptor Gene Is the Major Determinant of Common Early-Onset Androgenetic Alopecia. American Journal of Human Genetics, 77(1), 140. https://doi.org/10.1086/431425
- 7Cuevas-Diaz Duran, R., Martinez-Ledesma, E., Garcia-Garcia, M., Gauzin, D. B., Sarro-Ramírez, A., Gonzalez-Carrillo, C., Rodríguez-Sardin, D., Fuentes, A., & Cardenas-Lopez, A. (2024). The Biology and Genomics of Human Hair Follicles: A Focus on Androgenetic Alopecia. International Journal of Molecular Sciences, 25(5), 2542. https://doi.org/10.3390/ijms25052542
- 8Gatherwright, J., Liu, M. T., Amirlak, B., Gliniak, C., Totonchi, A., & Guyuron, B. (2013). The contribution of endogenous and exogenous factors to male alopecia: a study of identical twins. Plastic and reconstructive surgery, 131(5), 794e801e. https://doi.org/10.1097/PRS.0b013e3182865ca9
- 9Liu, J., Luo, W., Hu, Z., Zhu, X., & Zhu, L. (2024). The causal relationship between gut microbiota and androgenetic alopecia: A Mendelian randomization study. Medicine, 103(52), e41106. https://doi.org/10.1097/MD.0000000000041106
- 10Henne, S. K., & Heilmann-Heimbach, S. (2023). Male-pattern hair loss: Comprehensive identification of the associated genes as a basis for understanding pathophysiology. Medizinische Genetik, 35(1), 3. https://doi.org/10.1515/medgen-2023-2003
- 11Bhat, Y. J., Latif, I., & Hassan, I. (2020). Female Pattern Hair Loss—An Update. Indian Dermatology Online Journal, 11(4), 493.
- 12Kaliyadan, F. (2022). Androgenetic alopecia – medical management. Clinical Dermatology Review, 6(2), 75–79. https://doi.org/10.4103/cdr.cdr_27_21
- 13Asad, N., Naseer, M., & Ghafoor, R. (2024). Efficacy of Topical Finasteride 0.25% With Minoxidil 5% Versus Topical Minoxidil 5% Alone in Treatment of Male Pattern Androgenic Alopecia. Journal of drugs in dermatology: JDD, 23(11), 1003–1008.
- 14Liu, K. H., Liu, D., Chen, Y. T., & Chin, S. Y. (2019). Comparative effectiveness of low-level laser therapy for adult androgenic alopecia: a systematic review and meta-analysis of randomized controlled trials. Lasers in medical science, 34(6), 1063–1069. https://doi.org/10.1007/s10103-019-02723-6
- 15Bazmi, S., Sepehrinia, M., Pourmontaseri, H., Bazyar, H., Vahid, F., Farjam, M., Dehghan, A., Hébert, J. R., Homayounfar, R., & Shakouri, N. (2024). Androgenic alopecia is associated with a higher dietary inflammatory index and a lower antioxidant index score. Frontiers in Nutrition, 11, 1433962.
