When the body takes in a dangerous dose of ionizing radiation often within a matter of minutes or hours, it results in a full-blown medical crisis. This condition is called radiation sickness (medically: Acute Radiation Syndrome or ARS). Without prompt, specialized treatment, radiation sickness can be fatal.
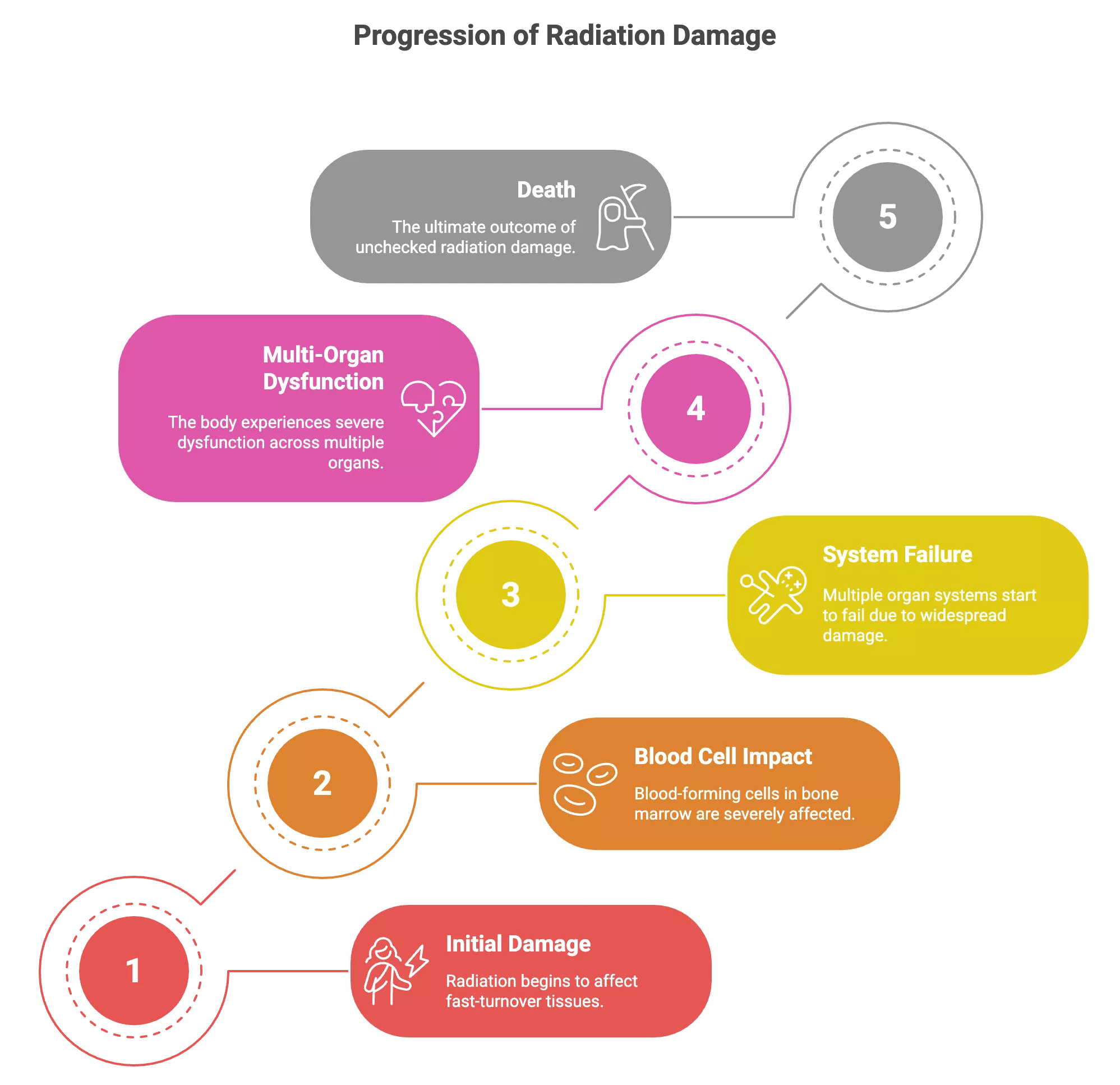
Radiation sickness develops very fast. The radiation is so dangerous because it immediately affects rapidly dividing cells of the body, like in the bone marrow, gastrointestinal lining, and skin.
Radiation sickness is not a very common condition. It’s usually a result of nuclear accidents, radiological terrorism, or malfunctions in radiation therapy. Early recognition is critical for proper management and survival; without it, radiation sickness can be fatal within hours to days. There is often already internal cellular death occurring even when the vital signs remain normal.
What Causes Radiation Sickness?
Most instances of radiation sickness have been well-known, which puts into perspective how uncommon high-dose exposure is, but the cause can be:
- Nuclear accidents (e.g., Chernobyl, Fukushima)
- Detonation of nuclear weapons or radiological terrorism
- Improper or accidental exposure during radiation therapy
- Occupational accidents in medical, research, or industrial settings
The risk and severity depend on the total radiation dose absorbed, the duration of exposure, and which parts of the body are affected. Generally speaking, full-body exposure to >1 Gray (Gy) of ionizing radiation can trigger acute radiation syndrome (ARS).1Macià I Garau, M., Lucas Calduch, A., & López, E. C. (2011). Radiobiology of the acute radiation syndrome. Reports of practical oncology and radiotherapy : journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology, 16(4), 123–130. https://doi.org/10.1016/j.rpor.2011.06.001
| Radiation Dose (Gy) | Expected Effects | Prognosis |
| 0.1–0.5 | No symptoms or mild changes in blood counts | Excellent |
| 0.5–1 | Mild symptoms; decreased lymphocytes | Likely recovery |
| 1–2 | Moderate symptoms; bone marrow suppression | Good with care |
| 2–6 | Severe symptoms; hematologic + GI syndrome | Possible with intensive care |
| 6–8 | Severe illness; survival unlikely without marrow transplant | Poor |
| >8 | Multi-organ failure within days | Fatal in most cases |
How does Radiation Damage the Body?
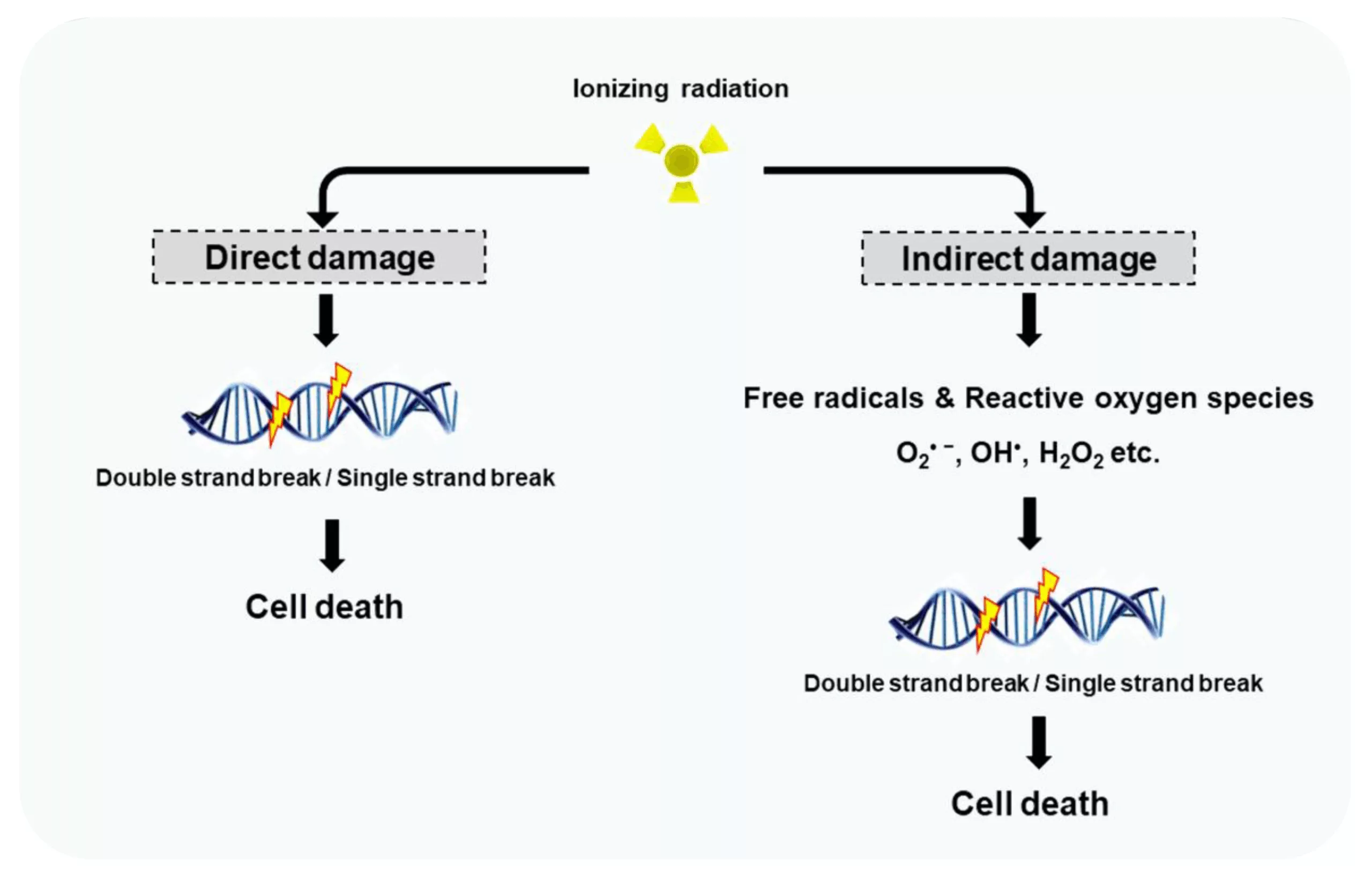
Ionizing radiation harms the body by breaking chemical bonds inside cells. It disrupts DNA, proteins, and membranes. The two main ways this damage happens:
- Direct Ionization: Radiation directly strikes DNA or vital cell components, breaking molecular structures and leading to mutations or cell death.
- Indirect Damage via Free Radicals: Radiation interacts with water inside the cells, and releases free radicals. These radicals attack DNA and cell structures.
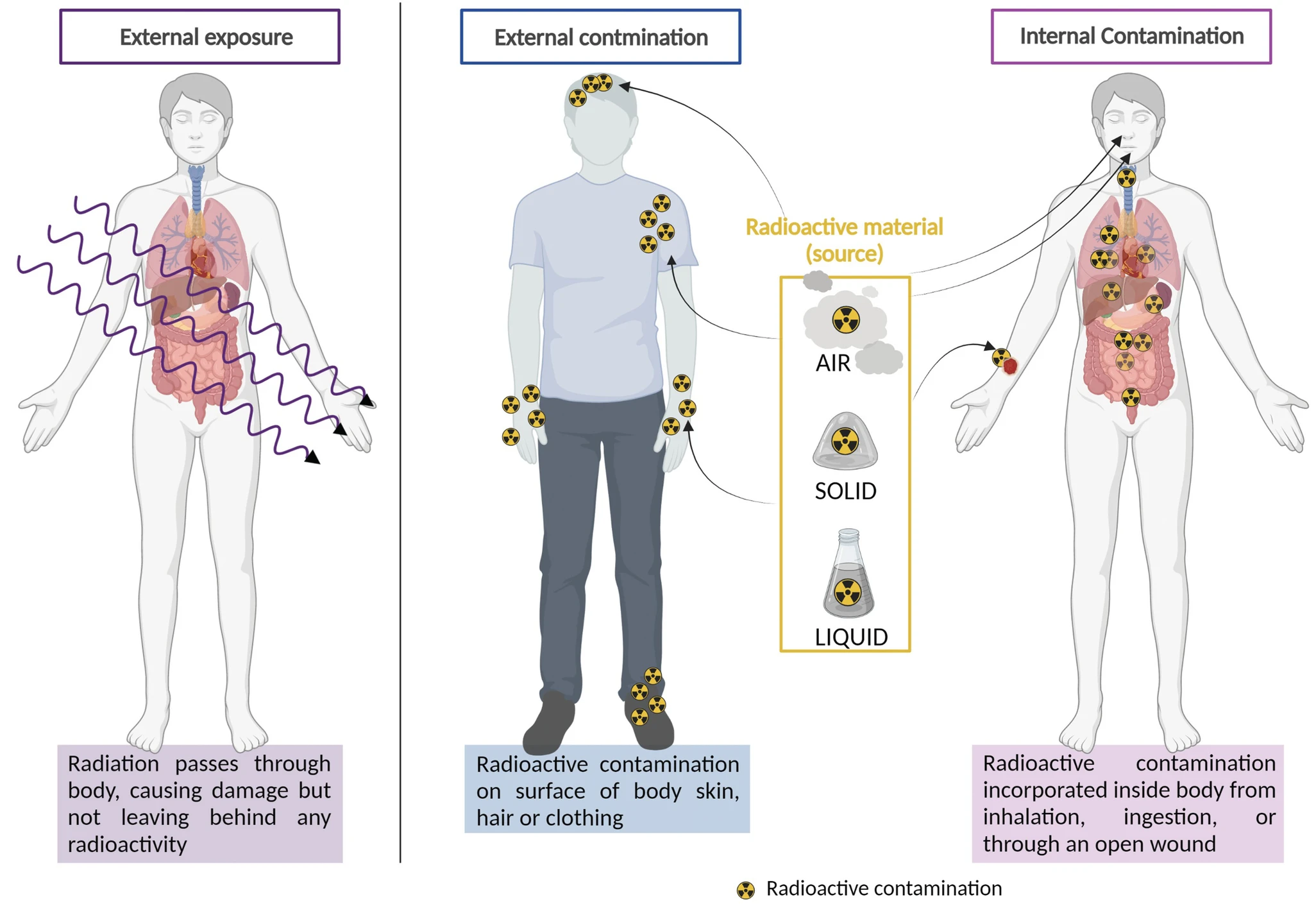
Radiation Exposure vs. Contamination: What’s the Difference?
When dealing with radiation emergencies, it’s important to understand two often-confused terms: radiation exposure and radiation contamination. No, they are not the same, and the response differs significantly.2Bushberg, J. T. (2025). Radiation Exposure and Contamination (Vol. 2025). MSD Manual. https://www.msdmanuals.com/professional/injuries-poisoning/radiation-exposure-and-contamination/radiation-exposure-and-contamination
| Concept | Radiation Exposure | Radiation Contamination |
| What it means | You were near a radiation source and received a dose of radiation | Radioactive material is on your skin, clothes, or inside your body |
| Is it radioactive? | No. Exposed people are not “radioactive.” | Yes. Contaminated people or objects can emit radiation |
| Can it spread? | No — exposure cannot be “passed on” | Yes — contamination can spread to others or the environment |
| Examples | Standing near a radioactive machine or reactor | Inhaling radioactive dust or ingesting contaminated food |
| Decontamination? | Not required unless contaminated | Required — involves removing clothes and washing body |
Symptoms of Radiation Sickness
Symptoms of radiation sickness appear in a very specific pattern. They can appear within minutes to hours, and may worsen over days without treatment. Recognizing these signs helps doctors provide better treatment.
Early Warning Signs (Hours to Days):
The first symptoms often feel like severe flu or food poisoning:
- Nausea and vomiting (often within 1–2 hours of exposure)
- Fatigue and weakness
- Headache
- Skin redness or irritation (similar to sunburn)
- Loss of appetite
- Diarrhea
Serious Complications:
As the disease advances, there may be other more severe symptoms. The following symptoms mean that there has been a lot of internal damage and signal an urgent need for intervention.
- Bleeding from the mouth, nose, or under the skin
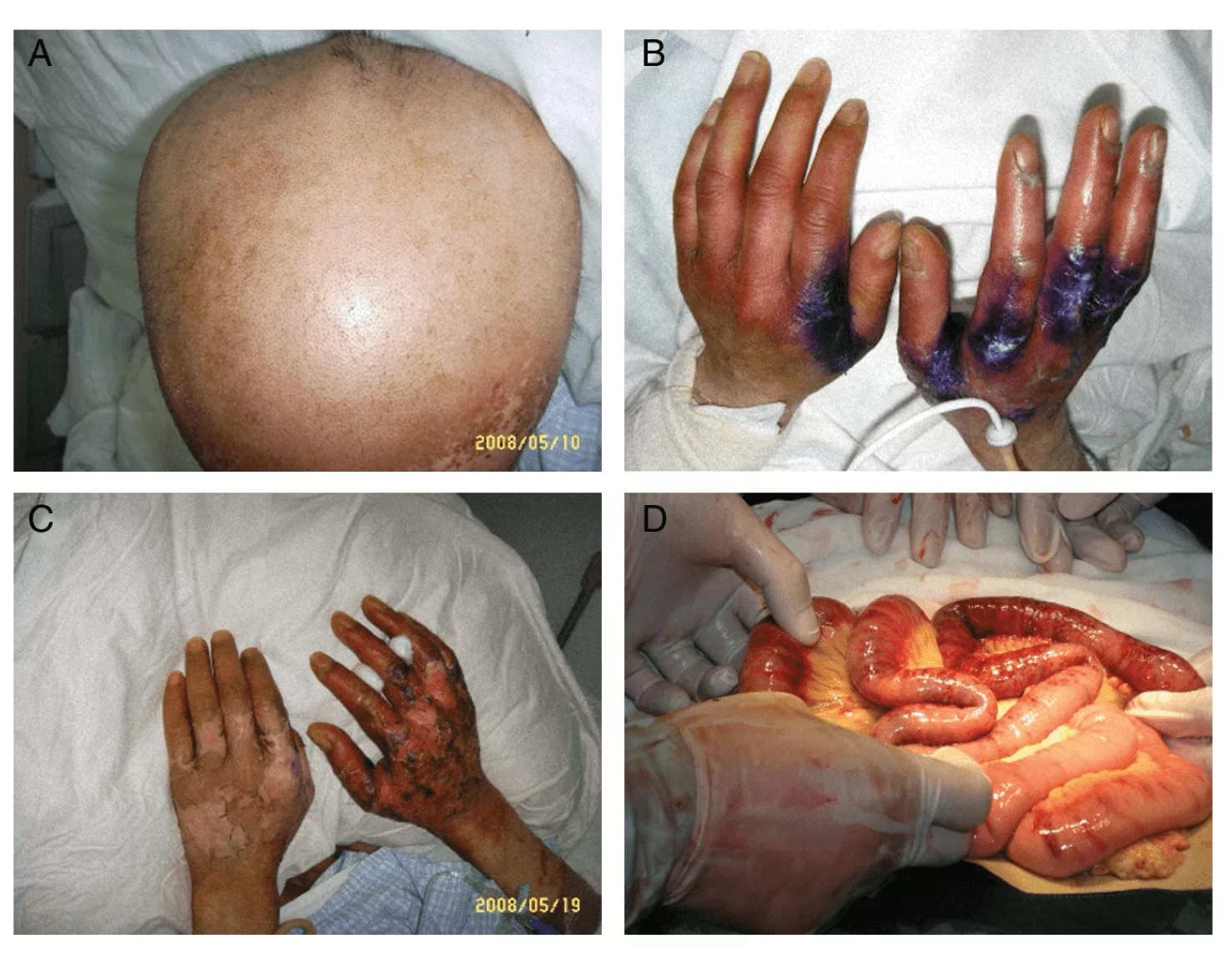
- Loss of hair in areas exposed to radiation
- Peeling of the skin, shedding of skin, and formation of blisters
- Frequent infections (due to weakened immunity)
- Low blood cell counts (anemia, leukopenia, thrombocytopenia)
- Confusion, dizziness, or seizures in the later stages
- Severe, persistent diarrhea
- Difficulty in breathing, and then eventually failure of the organs.
Rapid onset of nausea, vomiting, or neurological symptoms within minutes suggests a high dose of radiation and is a poor prognostic sign.
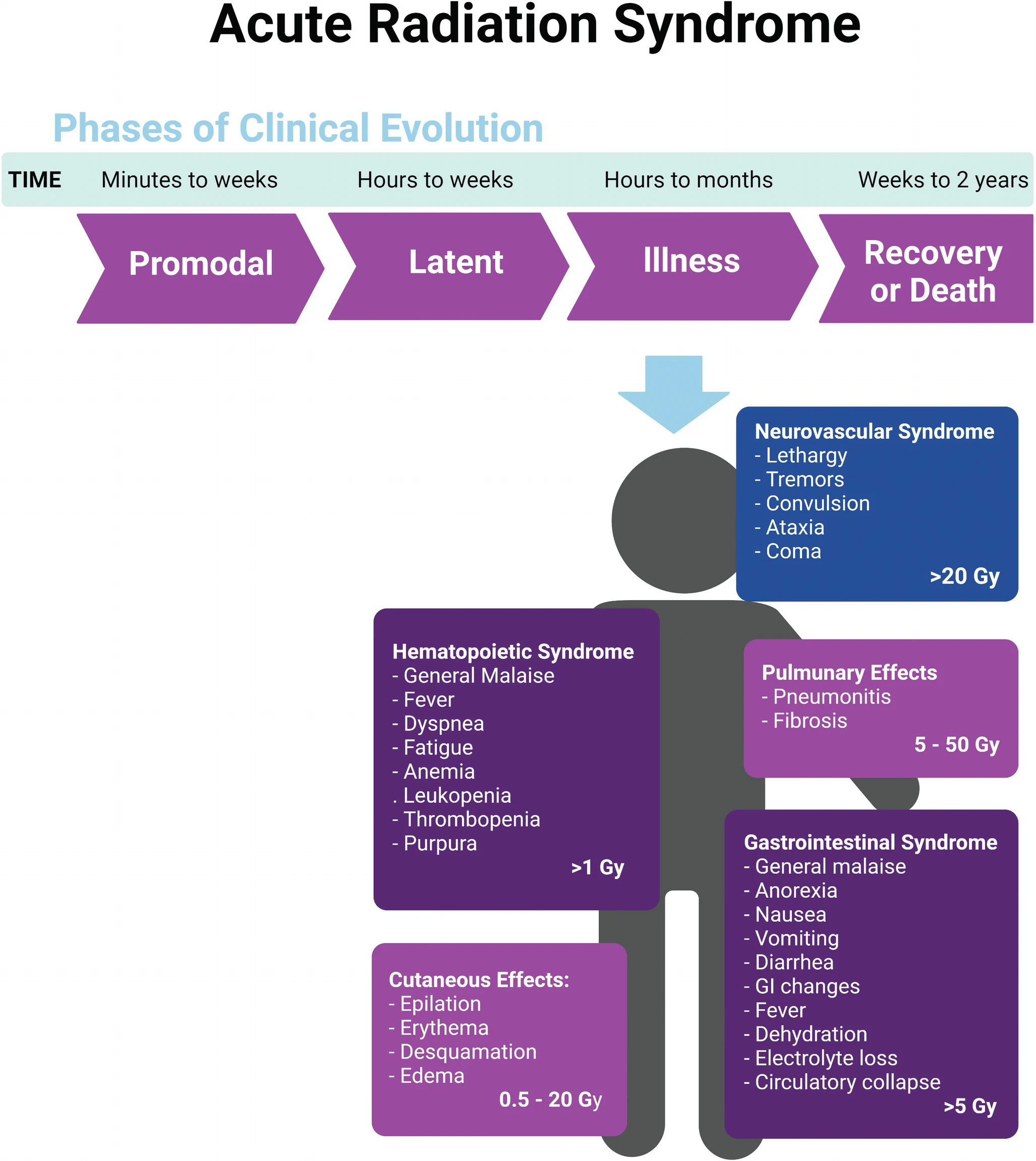
Stages of Radiation Sickness
Radiation sickness usually has four distinct phases of clinical illness.3Macià I Garau, M., Lucas Calduch, A., & López, E. C. (2011). Radiobiology of the acute radiation syndrome. Reports of practical oncology and radiotherapy: journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology, 16(4), 123–130. https://doi.org/10.1016/j.rpor.2011.06.001 The time of onset and the severity of the four phases depend on the received dose of radiation, the route of exposure, and the underlying health of the individual.
Stage 1: Initial Sickness (Prodromal Stage):
This is the body’s initial reaction to radiation within the first few hours of exposure.
- Symptoms: Nausea, vomiting, anorexia, fatigue, headache
- Higher doses lead to more rapid and severe onset.
- It may last a few hours to a few days.
Stage 2: Feeling Better (Latent Stage):
Deceivingly, within days, there is a “calm before the storm” with inconsequential improvement of symptoms.
- The patient feels well, yet there is increasingly advanced internal injury, particularly to the bone marrow and the lining of the GI tract.
- Duration is inversely related to dose: shortest with highest doses.
Stage 3: Severe Illness (Manifest Illness):
After a few days or weeks, the patient enters the critical period: symptoms return and intensify, and organ systems start failing. Based on the system affected most, there may be three kinds of symptoms:
- Hematopoietic symptoms (1–10 Gy): low blood counts, infections, bleeding
- Gastrointestinal syndrome (6–30 Gy): relentless diarrhea, dehydration, sepsis
- Neurovascular collapse (>30 Gy): confusion, seizures, coma — usually fatal in 1–3 days
Stage 4: Recovery or Death:
If a person survives in a critical state, he/she can expect gradual recovery over the next few months.
- Lower exposures: Recovery over an extended period with medical assistance
- Higher exposures: Organ failure is irreversible and ends in death
Diagnosis of Radiation Sickness
Diagnosing radiation sickness requires careful evaluation since early symptoms are nonspecific and can mimic infection, dehydration, or trauma. Accurate dose estimation and staging are essential for appropriate triage and treatment.
Clinical Assessment:
History taking is critical and should cover:
- Recent history of radiation exposure (occupational, medical, etc.)
- Type, duration, and estimated time of exposure
- Estimation of distance from the source of radiation
- Whether shielding or protective clothing was worn or not
Physical examination should assess:
- Vital signs and general condition
- Skin changes (burns, hair loss, etc.)
- Lymph node examination
- Neurological status
- Mucosal bleeding or petechiae
- Dehydration and signs of infection
Laboratory Tests:
Bone marrow and gut cells rapidly turn over, and are among the first to show evidence of damage so blood tests can help estimate exposure:
Complete Blood Count (CBC)4Macià I Garau, M., Lucas Calduch, A., & López, E. C. (2011). Radiobiology of the acute radiation syndrome. Reports of practical oncology and radiotherapy : journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology, 16(4), 123–130. https://doi.org/10.1016/j.rpor.2011.06.001
- Lymphocyte count drops within hours
- Neutropenia and thrombocytopenia develop later
- A decrease in red blood cell count appears over days
Blood Chemistry Panels
- Electrolyte imbalances
- Renal and liver function abnormalities
- Elevated inflammatory markers (e.g., CRP)
Specialized Tests
- Chromosome analysis (shows radiation damage)
- Dosimetry if radiation badges are available
- Biomarkers for radiation exposure (e.g., citrulline for GI injury)
Severity Assessment:
Doctors use the lymphocyte count to estimate dose:5Bushberg, J. T. (2025). Radiation Exposure and Contamination (Vol. 2025). MSD Manual. https://www.msdmanuals.com/professional/injuries-poisoning/radiation-exposure-and-contamination/radiation-exposure-and-contamination
| Lymphocyte Count | Radiation estimate |
| 1,500-4,000 cells/mm³ | Normal |
| 1,000-1,500 cells/mm³ at 48 hours | Mild exposure |
| 500-1,000 cells/mm³ at 48 hours | Moderate |
| 100-500 cells/mm³ at 48 hours | Severe |
| Less than 100 cells/mm³ at 48 hours | Very severe |
Time to vomiting also indicates severity:
| Clinical Indicator | Radiation Dose Estimate |
| Vomiting < 1 hour | Very high dose (>6–8 Gy) |
| Vomiting within 1–2 hrs | High dose (~3–6 Gy) |
| Vomiting after 2–6 hrs | Moderate dose (1–3 Gy) |
| Vomiting after >6 hrs | Lower dose (<1 Gy) |
Imaging Studies:
While not always necessary for diagnosis, imaging can give information about organ damage:
- Chest X-ray: Pneumonitis or pulmonary edema
- Abdominal CT or ultrasound: GI mucosal damage
- MRI: Bone marrow changes
Treatment of Radiation Sickness
Treatment of radiation sickness must start immediately. The focus at this stage is to support the body in the healing process, by using a combination of supportive care, targeted interventions, and contamination control.
Immediate Stabilization & Decontamination:
- Remove contaminated clothing
- Wash skin and wounds with soap and water
- Isolate patients to prevent contaminating healthcare workers and facilities
- Blood and urine samples for dosimetry prior to aggressive fluid administration
- Treat any life-threatening injuries (Trauma, burns, airway)
Hospital Care:
Radiation sickness affects multiple systems in phases; supportive care is the cornerstone of management.
Hematopoietic support
- Growth factors like Granulocyte colony-stimulating factor (G-CSF) to help bone marrow recover6Reeves G. (2014). Overview of use of G-CSF and GM-CSF in the treatment of acute radiation injury. Health physics, 106(6), 699–703. https://doi.org/10.1097/HP.0000000000000090
- Blood transfusions for severe anemia
- Platelet transfusions to prevent bleeding
Infection prevention
- Isolation to protect from infections
- Antibiotics, antifungals, and antivirals for infection prophylaxis
- Careful monitoring for any signs of infection
Gastrointestinal care
- IV fluid and electrolyte replacement to prevent dehydration
- Antiemetics for nausea and vomiting (e.g., ondansetron)
- Medications to control diarrhea
- Nutritional support: TPN or enteral feeding
- Broad-spectrum antibiotics to prevent sepsis
Specific Antidotes for Radioactive Isotopes:
Different radioactive materials require specific antidotes.7Yamamoto L. G. (2013). Risks and management of radiation exposure. Pediatric emergency care, 29(9), 1016–1029. https://doi.org/10.1097/PEC.0b013e3182a380b8 8Fukuda S. (2005). Chelating agents used for plutonium and uranium removal in radiation emergency medicine. Current medicinal chemistry, 12(23), 2765–2770. https://doi.org/10.2174/092986705774463012
| Isotope | Antidote | Notes |
| Cesium-137 | Prussian Blue | Enhances fecal excretion |
| Radioiodine (I-131) | Potassium iodide (KI) | Blocks thyroid uptake (must be given early) |
| Plutonium, Americium, Curium | DTPA (Ca- or Zn-DTPA) | Chelates transuranic elements |
| Uranium | Sodium bicarbonate | Alkalinizes urine, reduces kidney toxicity |
Bone Marrow Transplantation:
While bone marrow transplant can be life-saving in the most severe cases of hematopoietic failure (i.e, unresponsive to G-CSF and transfusion), it is usually only performed in patients who received a moderate radiation dose, have no multi-organ failure, and are otherwise healthy.
Long-Term Management:
Full recovery from radiation sickness takes time and requires:
- Psychological support for PTSD, anxiety, and grief
- Regular blood tests for hematologic malignancies
- Wound care for skin injuries
- Physical therapy
- Cancer screening
Prognosis of Radiation Sickness
The amount of radiation absorbed is overwhelmingly the largest factor for survival. Large doses (>10 Gy whole body) will result in certain death. Lower doses (1-2 Gy) still provide a high rate of recovery with aggressive treatment. Long-term survivors still suffer substantially increased rates of cancer and other diseases.9Kamiya, K., Ozasa, K., Akiba, S., Niwa, O., Kodama, K., Takamura, N., Zaharieva, E. K., Kimura, Y., & Wakeford, R. (2015). Long-term effects of radiation exposure on health. Lancet (London, England), 386(9992), 469–478. https://doi.org/10.1016/S0140-6736(15)61167-9
Prevention of Radiation Sickness
The only sure way to prevent ARS is to avoid high-dose exposure. The principle “ALARA” (As Low As Reasonably Achievable) guides radiation safety.10Mendonça, R. P., Estrela, C., Bueno, M. R., Carvalho, T. C. A. S. G., Estrela, L. R. A., & Chilvarquer, I. (2025). Principles of radiological protection and application of ALARA, ALADA, and ALADAIP: a critical review. Brazilian oral research, 39, e14. https://doi.org/10.1590/1807-3107bor-2025.vol39.014
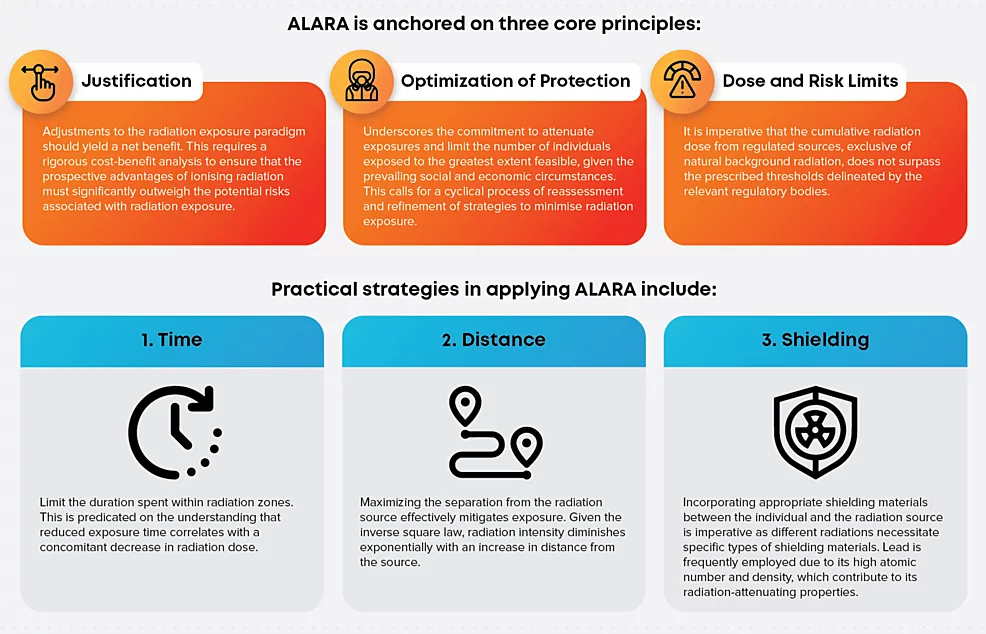
Radiation Safety Protocols:
- Proper shielding, distance, and exposure time limits
- Use of dosimeters and personal protective equipment (PPE)
- Regular training for healthcare providers, nuclear workers, and emergency responders.
Public Health & Emergency Preparedness:
- Stockpiling emergency supplies, especially potassium iodide (for iodine exposures), Prussian blue, DTPA.
- Public education on evacuation, decontamination, and shelter-in-place guidelines during nuclear events.
- Designated radiation emergency centers with decontamination facilities.
- Emergency drills for populations living near nuclear facilities
When to Seek Medical Help?
Get immediate emergency medical care if:
- You were near a radiation accident, even if you don’t notice symptoms yet
- You have severe nausea after a possible exposure
- You develop sudden, severe symptoms
- You find unusual materials that might be radioactive
Conclusion
Radiation sickness might seem like something from a disaster movie, but it’s a real medical emergency that requires immediate action. It can escalate quickly from vague symptoms to life-threatening organ failure, especially without emergency intervention. If you think you’ve been exposed to radiation, don’t delay: seek medical treatment immediately.
As nuclear technology evolves and becomes global, awareness and preparedness for radiation exposure become increasingly vital for both medical professionals and the public.
Refrences
- 1Macià I Garau, M., Lucas Calduch, A., & López, E. C. (2011). Radiobiology of the acute radiation syndrome. Reports of practical oncology and radiotherapy : journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology, 16(4), 123–130. https://doi.org/10.1016/j.rpor.2011.06.001
- 2Bushberg, J. T. (2025). Radiation Exposure and Contamination (Vol. 2025). MSD Manual. https://www.msdmanuals.com/professional/injuries-poisoning/radiation-exposure-and-contamination/radiation-exposure-and-contamination
- 3Macià I Garau, M., Lucas Calduch, A., & López, E. C. (2011). Radiobiology of the acute radiation syndrome. Reports of practical oncology and radiotherapy: journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology, 16(4), 123–130. https://doi.org/10.1016/j.rpor.2011.06.001
- 4Macià I Garau, M., Lucas Calduch, A., & López, E. C. (2011). Radiobiology of the acute radiation syndrome. Reports of practical oncology and radiotherapy : journal of Greatpoland Cancer Center in Poznan and Polish Society of Radiation Oncology, 16(4), 123–130. https://doi.org/10.1016/j.rpor.2011.06.001
- 5Bushberg, J. T. (2025). Radiation Exposure and Contamination (Vol. 2025). MSD Manual. https://www.msdmanuals.com/professional/injuries-poisoning/radiation-exposure-and-contamination/radiation-exposure-and-contamination
- 6Reeves G. (2014). Overview of use of G-CSF and GM-CSF in the treatment of acute radiation injury. Health physics, 106(6), 699–703. https://doi.org/10.1097/HP.0000000000000090
- 7Yamamoto L. G. (2013). Risks and management of radiation exposure. Pediatric emergency care, 29(9), 1016–1029. https://doi.org/10.1097/PEC.0b013e3182a380b8
- 8Fukuda S. (2005). Chelating agents used for plutonium and uranium removal in radiation emergency medicine. Current medicinal chemistry, 12(23), 2765–2770. https://doi.org/10.2174/092986705774463012
- 9Kamiya, K., Ozasa, K., Akiba, S., Niwa, O., Kodama, K., Takamura, N., Zaharieva, E. K., Kimura, Y., & Wakeford, R. (2015). Long-term effects of radiation exposure on health. Lancet (London, England), 386(9992), 469–478. https://doi.org/10.1016/S0140-6736(15)61167-9
- 10Mendonça, R. P., Estrela, C., Bueno, M. R., Carvalho, T. C. A. S. G., Estrela, L. R. A., & Chilvarquer, I. (2025). Principles of radiological protection and application of ALARA, ALADA, and ALADAIP: a critical review. Brazilian oral research, 39, e14. https://doi.org/10.1590/1807-3107bor-2025.vol39.014
