
What is Seborrheic Keratosis?
Seborrheic keratosis is a common benign skin growth made up of immature epidermal keratinocytes. It typically appears in adults and older individuals. These growths vary in appearance — from lightly pigmented patches to darker, scaly plaques that often look like they’re “stuck on” the skin. Although harmless and usually asymptomatic, many people seek removal for cosmetic reasons. Accurate diagnosis is essential to distinguish it from malignant lesions such as melanoma.1Greco, M. J., & Bhutta, B. S. (2023). Seborrheic Keratosis. In StatPearls. StatPearls Publishing.
Its prevalence rises with age, approaching 100 percent in those over 60 years old.2Yeatman JM, Kilkenny M, Marks R. The prevalence of seborrhoeic keratoses in an Australian population: does exposure to sunlight play a part in their frequency? Br J Dermatol. 1997 Sep;137(3):411-4. PMID: 9349339. It is also referred to as commonly referred to as age spots or senile warts.
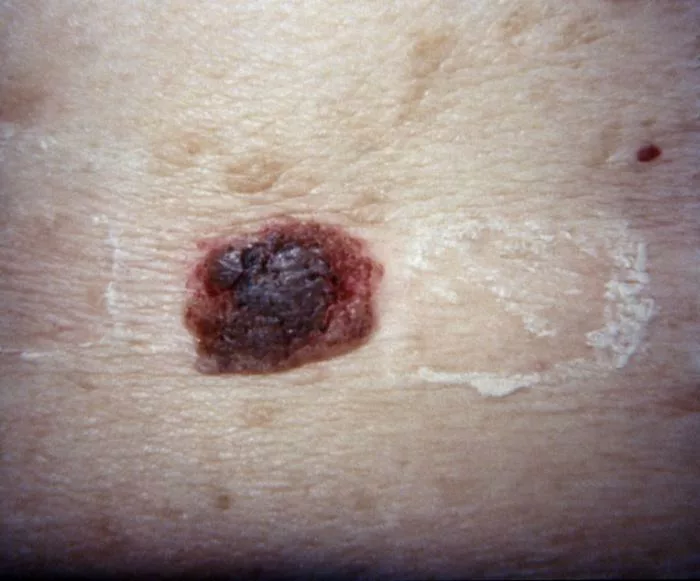
Image Courtesy: PHIL
Causes of Seborrheic Keratosis
Seborrheic keratosis3Barthelmann, S., Butsch, F., Lang, B. M., Stege, H., Großmann, B., Schepler, H., & Grabbe, S. (2023). Seborrheic keratosis. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG, 21(3), 265–277. https://doi.org/10.1111/ddg.14984 has a vast etiology. Although the exact mechanisms are not fully understood, several factors may contribute to its development. Some are discussed below:
Genetic Role:
Seborrheic keratosis tends to run in families, suggesting a genetic component to its development. Certain genetic variants, particularly in the fibroblast growth factor receptor 3 (FGFR3) and PIK3CA oncogenes, have been found in SK lesions, though their exact role in disease development remains unclear.4Hafner C, López-Knowles E, Luis NM, Toll A, Baselga E, Fernández-Casado A, Hernández S, Ribé A, Mentzel T, Stoehr R, Hofstaedter F, Landthaler M, Vogt T, Pujol RM, Hartmann A, Real FX. Oncogenic PIK3CA mutations occur in epidermal nevi and seborrheic keratoses with a characteristic mutation pattern. Proc Natl Acad Sci U S A. 2007 Aug 14;104(33):13450-4. doi: 10.1073/pnas.0705218104. Epub 2007 Aug 2. PMID: 17673550; PMCID: PMC1948900.
This genetic predisposition can result in a higher prevalence of SK within families, and it may be passed down through generations.5Barthelmann, S., Butsch, F., Lang, B. M., Stege, H., Großmann, B., Schepler, H., & Grabbe, S. (2023). Seborrheic keratosis. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG, 21(3), 265–277. https://doi.org/10.1111/ddg.14984
Age & Prevalence:
SK becomes more common with age, particularly in individuals over 40, though it can also affect younger individuals. It is more prevalent in the elderly, but teenagers and young adults can also develop the condition. While there is some evidence suggesting that the condition may be more frequent in males, the overall prevalence increases with age in both genders.6Gorai, S., Ahmad, S., Raza, S. S. M., Khan, H. D., Raza, M. A., Etaee, F., Cockerell, C. J., Apalla, Z., & Goldust, M. (2022). Update of pathophysiology and treatment options of seborrheic keratosis. Dermatologic therapy, 35(12), e15934. https://doi.org/10.1111/dth.15934
Human Papilloma Virus:
There is limited evidence suggesting a potential link between certain types of HPV, particularly HPV type 20, and the development of seborrheic keratosis. However, this association is rare, and further research is needed to clarify the role of HPV in SK. Zinc oxide ointments have a curative effect in such situations.7Kondo, M., Matsushima, Y., Nakanishi, T., Iida, S., Habe, K., & Yamanaka, K. (2023). Seborrheic Keratosis Caused by Human Papillomavirus Type 20 Ameliorated by Zinc Oxide Ointment. Clinics and practice, 13(2), 367–371. https://doi.org/10.3390/clinpract13020033
Ultraviolet Radiations:
Extreme sun exposure may cause this growth. Sunlight is a source of Ultraviolet radiation. These UV radiations may cause this condition in certain individuals. Some studies suggest that UV exposure may activate genetic mutations, such as those in the FGFR3 gene, which could contribute to the development of SK.8Kwon OS, Hwang EJ, Bae JH, Park HE, Lee JC, Youn JI, Chung JH. Seborrheic keratosis in the Korean males: causative role of sunlight. Photodermatol Photoimmunol Photomed. 2003 Apr;19(2):73-80. doi: 10.1034/j.1600-0781.2003.00025.x. PMID: 12945806.
Symptoms
Seborrheic keratosis (SK) is usually painless and doesn’t cause any symptoms. The lesions typically look like they’re stuck on the skin, with a scaly or rough texture. They can range in color from light tan to brown or black, and often have a dull surface with small, plugged hair follicles, giving them a wrinkled appearance. Early SK lesions often start as flat, light brown, or skin-colored spots that resemble freckles or lentigines.9Karadag, A. S., & Parish, L. C. (2018). The status of the seborrheic keratosis. Clinics in dermatology, 36(2), 275–277. https://doi.org/10.1016/j.clindermatol.2017.09.011
While most seborrheic keratoses are asymptomatic, they may cause irritation or discomfort if inflamed or subjected to friction, particularly in skin folds or areas that experience persistent rubbing from clothing. In such cases, SKs may be associated with mild pain or pruritus (itching). It is always advisable to seek professional help to evaluate the condition and differentiate it from other malignant lesions.
Location & Distribution:
SKs can develop anywhere on the body, except for the palms and soles. The number of lesions can range from just one to hundreds. You’ll typically see them on the trunk, face, scalp, arms, and legs. In skin folds, such as under the breasts or in the groin, they may form pedunculated lesions (with a stalk).
Clinical Variants:
While most of the lesions share similar characteristics, there are several clinical variants that differ in appearance and location.10UpToDate. (n.d.). Seborrheic keratosis. Retrieved April 9, 2025, from https://www.uptodate.com/contents/seborrheic-keratosis?search=seborrheic%20keratosis&source=search_result&selectedTitle=1%7E43&usage_type=default&display_rank=1#H1726880976 Some notable ones are mentioned below:
- Stucco Keratosis: This variant consists of small, white, fine, stuck-on papules, usually found on the ankles and dorsum of the feet.
- Dermatosis Papulosa Nigra: Common in individuals with darkly pigmented skin, this variant presents with acanthotic, brown to black papules primarily located on the face and neck, with the number of lesions increasing with age.
Diagnosis of Seborrheic Keratosis
The diagnosis is primarily clinical, based on its distinctive appearance as a stuck-on, scaly, brown to black, adherent papule. Experienced clinicians can usually recognize SK based on these characteristics. However, dermoscopy can further support the diagnosis when necessary.11Minagawa A. (2017). Dermoscopy-pathology relationship in seborrheic keratosis. The Journal of Dermatology, 44(5), 518–524. https://doi.org/10.1111/1346-8138.13657
Dermoscopy:
Dermoscopy is a non-invasive diagnostic technique where healthcare providers use a dermatoscope (a handheld instrument) to examine the lesion. This tool helps reveal details that are not visible to the naked eye, aiding in the identification of seborrheic keratosis morphology. Dermoscopic features typical of SK include:
- Milia-like Cysts: These are very small whitish-yellow fluid-filled cysts.
- Crypts & Furrows: The crypts and furrows form a warty appearance of seborrheic keratosis.
- Keratin Plugs: In certain cases, keratin plugs are present in brownish or yellowish structures
- Well-Defined Borders: Unlike cancerous and pre-cancerous lesions, these lesions have a well-defined and demarcated border.
Therefore, these features clearly help in the differentiation between pre-cancerous lesions and seborrheic keratosis.
Biopsy & Histopathology:
A biopsy is generally not required for the diagnosis of SK. However, if the clinical or dermoscopic appearance is unclear, or if there is concern about malignancy, a biopsy may be performed. The histopathologic examination of SK typically reveals well-demarcated intraepidermal proliferations of keratinocytes, often with papillomatosis, acanthosis, hyperkeratosis, and horn cysts.
In cases where the diagnosis remains uncertain, biopsy and histopathological analysis help rule out skin cancers such as melanoma, squamous cell carcinoma, or basal cell carcinoma.
Treatment of Seborrheic Keratosis
The treatment is pursued for aesthetic reasons, although treatment may also be sought if the lesions cause discomfort or irritation due to friction.12Wollina U. (2019). Recent advances in managing and understanding seborrheic keratosis. F1000Research, 8, F1000 Faculty Rev-1520. https://doi.org/10.12688/f1000research.18983.1 The choice of treatment varies depending on the patient’s needs, lesion characteristics, and physician recommendation. Common treatment options include:
Cryotherapy:
Cryotherapy or cryoablation is the choice of treatment when the lesions are small in size. Using liquid nitrogen achieves the freezing of the lesion’s growth, leading to its eventual sloughing off. One can apply liquid nitrogen for this purpose using a spray or a cotton-tip applicator.
Electrosurgery:
This procedure uses specialized instruments to cut or remove the lesion completely, often combined with curettage (scraping). Electrosurgery is particularly effective for larger or raised lesions.
Laser Therapy:
Laser is the most conservative treatment option. It heals with minimum scarring. It is usually chosen by the physician in situations where esthetics are of prime importance.
Shave Excision:
A scalpel is used to shave off the lesion from the surface of the skin. It may or may not result in the scarring.
Topical Treatments for Seborrheic Keratosis:
Several topical agents have been explored for the treatment of SK, though their efficacy is generally limited. These include:
40% Hydrogen Peroxide (HP40)
Hydrogen peroxide is commonly used in lower concentrations for skin disinfection, but at a 40% concentration, it may help treat seborrheic keratosis by breaking down the lesion. However, the strength of HP40 may lead to irritation, and it should be used cautiously. Despite its potential drawbacks, it offers a promising alternative to surgical methods.13Hydrogen peroxide 40% (Eskata) for seborrheic keratoses. (2018). The Medical letter on drugs and therapeutics, 60(1556), 157–158.
Tazarotene 0.1% Ointment
A topical retinoid that has been evaluated for SK treatment with mixed results.
Aqueous Nitric Zinc Complex
Aqueous nitric zinc complex-containing products can be used as a topical treatment of seborrheic keratosis.14Lacarrubba, F., Nasca, M. R., Verzì, A. E., & Micali, G. (2017). A novel topical agent in the treatment of seborrheic keratoses: A proof of concept study by clinical and dermoscopic evaluation. Dermatologic therapy, 30(5), 10.1111/dth.12526. https://doi.org/10.1111/dth.12526
Differential Diagnosis
Actinic Keratosis vs. Seborrheic Keratosis:
Actinic keratosis (AK)15Reinehr, C. P. H., & Bakos, R. M. (2019). Actinic keratoses: review of clinical, dermoscopic, and therapeutic aspects. Anais brasileiros de dermatologia, 94(6), 637–657. https://doi.org/10.1016/j.abd.2019.10.004 and seborrheic keratosis (SK) are both types of keratosis but differ significantly in terms of their nature and potential risks. Unlike seborrheic keratosis, actinic keratosis is a precancerous condition that has the potential to progress into squamous cell carcinoma (SCC), a type of skin cancer. Burning sensations are common in cases of actinic keratosis, especially when exposed to sunlight.
When a doctor suspects actinic keratosis, the most common diagnostic test is a biopsy. In contrast, seborrheic keratosis generally does not require a biopsy unless there are concerns about malignancy. While genetic factors play a significant role in the development of seborrheic keratosis, they have a minimal impact on the formation of actinic keratosis, which is primarily linked to sun exposure and ultraviolet (UV) radiation.
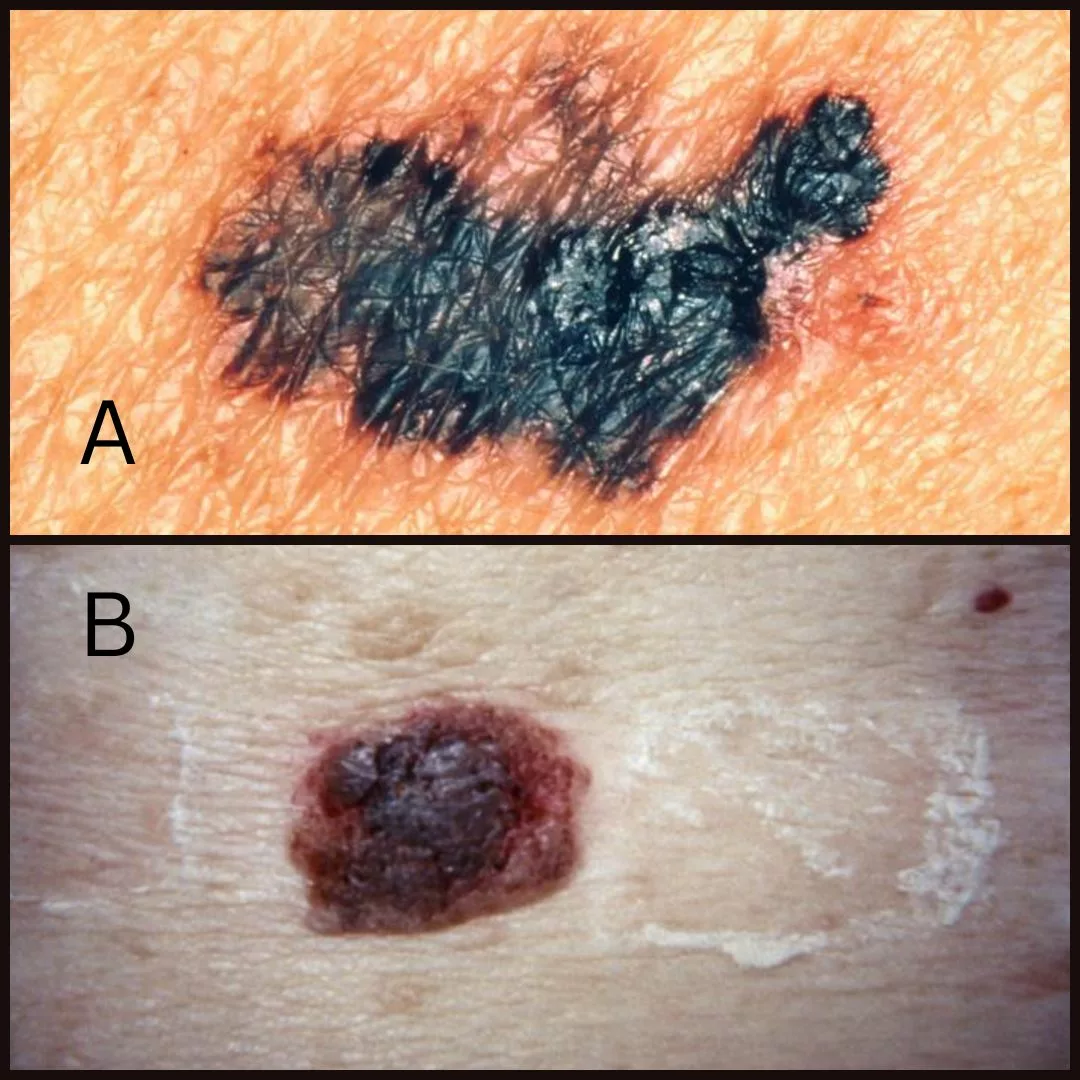
Melanoma Vs. Seborrheic Keratosis:
Seborrheic keratosis may resemble melanoma in appearance, but they are distinct in terms of pathophysiology, treatment, and prognosis. While seborrheic keratosis is a benign, non-cancerous growth, melanoma is a type of skin cancer and can be life-threatening if not detected and treated early.
Seborrheic keratosis is often misdiagnosed as melanoma due to its similar looks, presenting a diagnostic challenge. The definitive way to differentiate between the two is through a biopsy, which helps confirm the diagnosis and determine the appropriate course of action for treatment.16Janowska, A., Oranges, T., Iannone, M., Romanelli, M., & Dini, V. (2021). Seborrheic keratosis-like melanoma: a diagnostic challenge. Melanoma Research, 31(5), 407–412. https://doi.org/10.1097/CMR.0000000000000756
Skin Tags Vs. Seborrheic Keratosis:
Seborrheic keratosis and Skin tags (Acrochordon) may appear similar at first glance, but they’re quite different in terms of structure and appearance. Skin tags are small, soft growths made mostly of collagen fibers and blood vessels, often hanging off the skin by a stalk. On the other hand, seborrheic keratosis is a rough, scaly growth made of keratin and keratinocytes, and it can range in color from tan to black due to melanin. While both are typically benign, the texture of seborrheic keratosis is much rougher, and it tends to be more firmly attached to the skin.

Take Home Message
To sum it up, this is a condition of aesthetic importance. Being asymptomatic and painless, it rarely requires treatment. However, it may vary in its appearance from patient to patient. People often confuse it with melanoma. To differentiate between seborrheic keratosis and melanoma, physicians can perform biopsy and dermoscopy diagnostic tests.
Refrences
- 1Greco, M. J., & Bhutta, B. S. (2023). Seborrheic Keratosis. In StatPearls. StatPearls Publishing.
- 2Yeatman JM, Kilkenny M, Marks R. The prevalence of seborrhoeic keratoses in an Australian population: does exposure to sunlight play a part in their frequency? Br J Dermatol. 1997 Sep;137(3):411-4. PMID: 9349339.
- 3Barthelmann, S., Butsch, F., Lang, B. M., Stege, H., Großmann, B., Schepler, H., & Grabbe, S. (2023). Seborrheic keratosis. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG, 21(3), 265–277. https://doi.org/10.1111/ddg.14984
- 4Hafner C, López-Knowles E, Luis NM, Toll A, Baselga E, Fernández-Casado A, Hernández S, Ribé A, Mentzel T, Stoehr R, Hofstaedter F, Landthaler M, Vogt T, Pujol RM, Hartmann A, Real FX. Oncogenic PIK3CA mutations occur in epidermal nevi and seborrheic keratoses with a characteristic mutation pattern. Proc Natl Acad Sci U S A. 2007 Aug 14;104(33):13450-4. doi: 10.1073/pnas.0705218104. Epub 2007 Aug 2. PMID: 17673550; PMCID: PMC1948900.
- 5Barthelmann, S., Butsch, F., Lang, B. M., Stege, H., Großmann, B., Schepler, H., & Grabbe, S. (2023). Seborrheic keratosis. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG, 21(3), 265–277. https://doi.org/10.1111/ddg.14984
- 6Gorai, S., Ahmad, S., Raza, S. S. M., Khan, H. D., Raza, M. A., Etaee, F., Cockerell, C. J., Apalla, Z., & Goldust, M. (2022). Update of pathophysiology and treatment options of seborrheic keratosis. Dermatologic therapy, 35(12), e15934. https://doi.org/10.1111/dth.15934
- 7Kondo, M., Matsushima, Y., Nakanishi, T., Iida, S., Habe, K., & Yamanaka, K. (2023). Seborrheic Keratosis Caused by Human Papillomavirus Type 20 Ameliorated by Zinc Oxide Ointment. Clinics and practice, 13(2), 367–371. https://doi.org/10.3390/clinpract13020033
- 8Kwon OS, Hwang EJ, Bae JH, Park HE, Lee JC, Youn JI, Chung JH. Seborrheic keratosis in the Korean males: causative role of sunlight. Photodermatol Photoimmunol Photomed. 2003 Apr;19(2):73-80. doi: 10.1034/j.1600-0781.2003.00025.x. PMID: 12945806.
- 9Karadag, A. S., & Parish, L. C. (2018). The status of the seborrheic keratosis. Clinics in dermatology, 36(2), 275–277. https://doi.org/10.1016/j.clindermatol.2017.09.011
- 10UpToDate. (n.d.). Seborrheic keratosis. Retrieved April 9, 2025, from https://www.uptodate.com/contents/seborrheic-keratosis?search=seborrheic%20keratosis&source=search_result&selectedTitle=1%7E43&usage_type=default&display_rank=1#H1726880976
- 11Minagawa A. (2017). Dermoscopy-pathology relationship in seborrheic keratosis. The Journal of Dermatology, 44(5), 518–524. https://doi.org/10.1111/1346-8138.13657
- 12Wollina U. (2019). Recent advances in managing and understanding seborrheic keratosis. F1000Research, 8, F1000 Faculty Rev-1520. https://doi.org/10.12688/f1000research.18983.1
- 13Hydrogen peroxide 40% (Eskata) for seborrheic keratoses. (2018). The Medical letter on drugs and therapeutics, 60(1556), 157–158.
- 14Lacarrubba, F., Nasca, M. R., Verzì, A. E., & Micali, G. (2017). A novel topical agent in the treatment of seborrheic keratoses: A proof of concept study by clinical and dermoscopic evaluation. Dermatologic therapy, 30(5), 10.1111/dth.12526. https://doi.org/10.1111/dth.12526
- 15Reinehr, C. P. H., & Bakos, R. M. (2019). Actinic keratoses: review of clinical, dermoscopic, and therapeutic aspects. Anais brasileiros de dermatologia, 94(6), 637–657. https://doi.org/10.1016/j.abd.2019.10.004
- 16Janowska, A., Oranges, T., Iannone, M., Romanelli, M., & Dini, V. (2021). Seborrheic keratosis-like melanoma: a diagnostic challenge. Melanoma Research, 31(5), 407–412. https://doi.org/10.1097/CMR.0000000000000756



