
Sigmoidoscopy is the minimally invasive diagnostic test used to examine the sigmoid colon. The sigmoid colon is the lower part of your large intestine or colon. This part of the colon is near to the rectum and anus. In this test, a thin, lighted tube is inserted through the anus and rectum into the colon to examine the areas.
There are two types of sigmoidoscopy: flexible sigmoidoscopy and rigid sigmoidoscopy. The flexible type uses a flexible endoscope, while rigid sigmoidoscopy uses a rigid diagnostic device. However, rigid sigmoidoscopy has poor patient acceptance and has not been as successful as flexible sigmoidoscopy. This test is being used to test several symptoms, but most importantly, it can help diagnose colorectal cancer and, hence, aid in the control of large bowel cancer.1Winawer, S. J., Miller, C., Lightdale, C., Herbert, E., Ephram, R. C., Gordon, L., & Miller, D. (1987). Patient response to sigmoidoscopy: a randomized, controlled trial of rigid and flexible sigmoidoscopy. Cancer, 60(8), 1905-1908.
Why is Sigmoidoscopy required?
Sigmoidoscopy is used to screen colon and rectal cancer cancers. It can also be used to take a tissue sample or biopsy. Additionally, it can diagnose and examine following certain conditions in the colon and rectum. The indications for sigmoidoscopy include:
- Ulcers
- Sores
- Hemorrhoids
- Polyps
- Tumors
- Strictures
- Diverticula
- Changes in bowel habits
- Itching around the anus
- Mucus or blood in the stool
Flexible Sigmoidoscopy
Flexible sigmoidoscopy is a video endoscope or flexible fiberoptic. These sigmoidoscopes are designed to examine the mucosal surfaces of the rectum and sigmoid colon. They are available in 35 cm and 60 cm lengths. The preferred length of the flexible sigmoidoscope is 60 cm, as it allows examination of the more significant part of the colon. Three types of these endoscopes are available: a disposable endoseath type, a video scope, and a fiberoptic scope. The technical design of the flexible sigmoidoscopy provides a more comfy examination for the patient. The longer length of this endoscope allows the examination of more parts of the colon. Adequate bowel preparations are required for satisfactory visualization of the colonic mucosa. Analgesics or sedation is usually not required during the flexible sigmoidoscopy. Nitrous oxide can reduce discomfort during this procedure.
The basic equipment required for routine flexible sigmoidoscopy are:
- A light source
- Sigmoidoscope
- Biopsy forceps
- Suction apparatus
- Irrigation apparatus
- Water
- Cytology brushes
- Lubricant
- Nonsterile gloves
- Washing receptacle
- Eyewear and protective gowns for operator
- A gown for the patient2Harper, M. B., & Pope, J. B. (1997). Flexible sigmoidoscopy. Primary Care: Clinics in Office Practice, 24(2), 341-357.
Rigid Sigmoidoscopy
The rigid sigmoidoscope is a self-lubricating, plastic, disposable instrument. It is 1.8 cm in diameter and 25 cm in length. Rigid sigmoidoscopy is usually done on patients without a prepared bowel. It is an easy-to-learn and comparatively safe technique. However, it has poor patient acceptance due to the discomfort experienced by the patients during the procedure. During this procedure, patients experience severe to moderate discomfort. Most of the discomfort is experienced at the first major turn of the rectosigmoid, which is at about 17 cm.
Additionally, the views are limited. Only one person can see and observe the sigmoid colon at a time, and it cannot create a visual record of the findings and observations. Visualizations of the sigmoid colon and rectosigmoid junction are unsuccessful in more than 30% of examinations. The average insertion depth of this sigmoidoscope by skilled physicians is only 20 cm or less.3Rao, V. S. R., Ahmad, N., Al‐Mukhtar, A., Stojkovic, S., Moore, P. J., & Ahmad, S. M. (2005). Comparison of rigid vs. flexible sigmoidoscopy in the detection of significant anorectal lesions. Colorectal Disease, 7(1), 61-64.
The basic equipment required for routine rigid sigmoidoscopy includes:
- A light source
- Protoscope
- Insufflation device
- Suction device
- Lubricant
- Filter
- Bellows
- Biopsy forceps
- Specimen container4Simpson, P. J., McMurrick, P. J., Polglase, A. L., & Koh, C. E. (2010). Comparison of equipment management and cleaning protocols for rigid sigmoidoscopy. ANZ Journal of Surgery, 80(10), 728-731.
Preparation of Sigmoidoscopy & Patient Preparation
This screening examination can be included in a routine hospital visit. However, appropriate preparation is necessary.
Medical History & Examination
The healthcare provider will look for your detailed medical history to document previous gastrointestinal complaints, diagnoses, and procedures. The provider will ask for the symptoms such as changes in bowel habits, bowel function, presence of rectal bleeding, chronic diarrhea, constipation, or tenesmus. The provider will also inquire about your abdominal symptoms, such as bloating, cramping, pain, distension, nausea, vomiting, early satiety, and decreased appetite. They will also look for general symptoms such as fever or decreased energy levels.5Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
Well-informed patients are more cooperative. The provider will thoroughly explain the procedure to the patient. After the discussion, written consent is obtained from the patient. After the consent, the provider will ask a few questions before the procedure. These questions include:
- Do you have a previous history of bleeding?
- Are you pregnant, or do you think you can be pregnant?
- What kind of medicines are you taking?
- Are you sensitive to any medicines?
- Are you taking any blood thinning medications?
- Blood-thinning drugs such as ibuprofen and aspirin must be stopped.
Bowel Preparation
The preparation process for the sigmoidoscopy is uncomfortable, but it is an essential component of a successful procedure. The provider will give some directions on preparing your bowel for sigmoidoscopy. Before the test, you will be given specific instructions about fasting or following a special diet. A high-fiber diet must be discontinued a few days before. Taking an enema, laxative, or rectal laxative would be best. The frequently used method is hypertonic phosphate enema. The provider will advise discontinuing all iron medication for 2 weeks before the examination. Iron can make the feces adhere to the bowel wall, leading to additional mucosal coating and incomplete assessment. Some other medicines that slow bowel function (such as codeine) must be discontinued.
Your bowel must be well cleaned. Sometimes, you may need to drink a special fluid that will help prepare your bowel. Mix Colyte is directed with water the day before the examination. Drink all between 2:00 p.m. and 6:00 p.m. and ensure all granules are dissolved. Consume it in at least an 8-ounce glass every 15 minutes; adding a small amount of ice will make it more palatable. Resume drinking the fluid until the bottle is empty.6Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
Patient Preparation & Positioning
You will be asked to remove your accessories or any other object that can interfere with the procedure. Additionally, you need to wear a hospital gown for this process. After that, you may be put in the knee-chest position, like kneeling with your head and chest bent down. The other position is to lie on your left side with your knees bent toward your chest.7Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
Procedure of Sigmoidoscopy
The procedure of the sigmoidoscopy can cause mild discomfort. You can have a brief muscle spasm or belly pain during the examination. You may also have a strong urge to have a bowel movement. However, taking deep breaths while tube insertion can help in decreasing the awkward feelings. The procedure of the sigmoidoscopy is as follows:
For a rectal examination to look for mucus, stool, or blood, the provider will first gently dilate the anus. The provider use a suction device to remove the liquid stool.
The provider will insert the lubricated tube in the anus slowly and will move it into the rectum and colon. The healthcare provider will remove the tube after a detailed examination of the lower part of the colon. Air may be injected into your stools to improve visibility during the exam.
A sigmoidoscopy may be done together with an anoscopy or a proctoscopy. If another test is done, a special tube will be inserted to check your lower rectum or anal canal.
During the examination, tissue samples can be taken from the lining of the large intestine with the help of forceps, swabs, and a special brush. Polyps less than 5 mm in diameter must be biopsied, but polyps that are greater in size (5 to 10 mm) are assumed to be adenomatous.8Zuber, T. J. (2001). Flexible sigmoidoscopy. American Family Physician, 63(7), 1375-1380.
After the Examination
After examination, you will be asked to expel all the gas. You may resume your everyday routine and diet. If you had a biopsy during the procedure, it will be sent to the pathological lab for further evaluation. Avoid weight lifting and straining for one week.
Abnormal Findings of Sigmoidoscopy
Abnormal findings of the sigmoidoscopy indicate severe gastrointestinal conditions. The abnormal findings include:
- Polyps
- Diverticulitis
- Hemorrhoids
- Anal fissures
- Inflammatory bowel diseases
- Cancer
Complications After Sigmoidoscopy
Although sigmoidoscopy is a safe procedure, it has several complications. These side effects of the sigmoidoscopy include:
- Severe bleeding
- Injuries in the colon
- Peritonitis
- A perforation in the intestinal wall
- Adverse reactions to bleeding
- Blood pressure changes
These events are rare (1 in 1000 cases). Other complications include:
- Rectal bleeding
- Pain
- Black stool
- Vomiting
- Fainting
- Fever
- Inability to have a bowel movement (for over two days).9Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
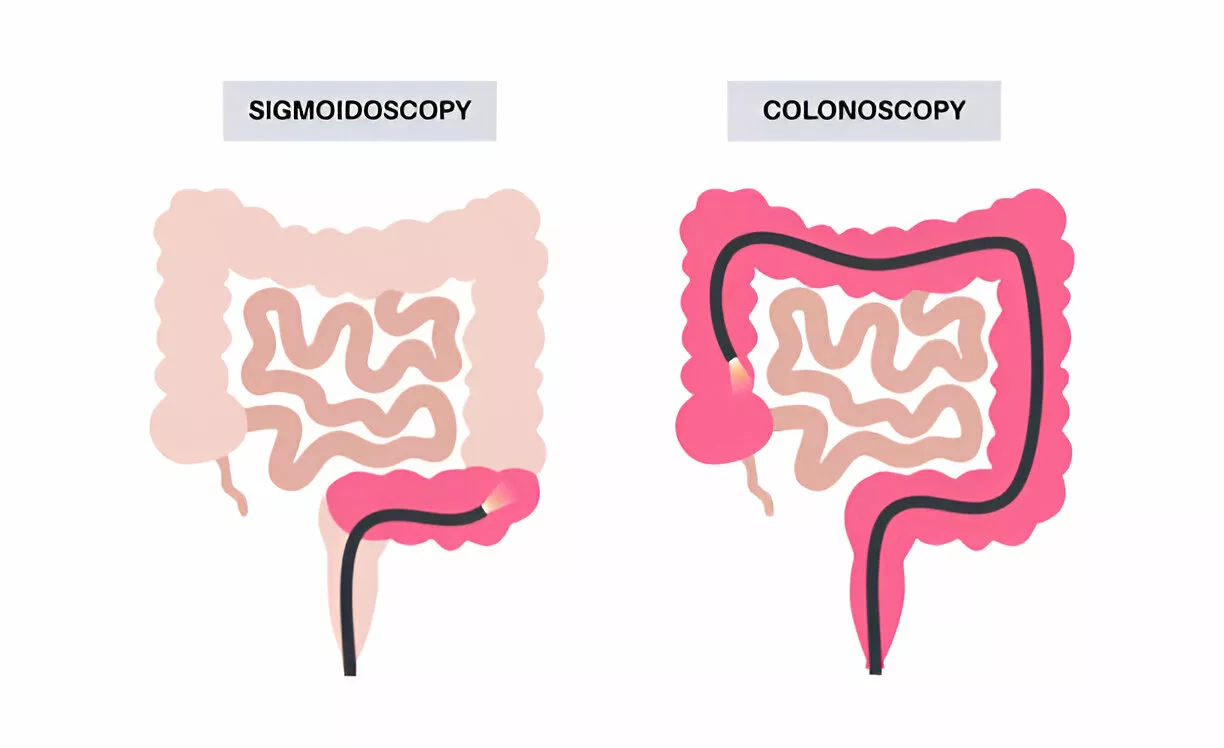
Sigmoidoscopy Versus Colonoscopy
Sigmoidoscopy involves the use of a shorter, flexible tube called a sigmoidoscope, which is equipped with a camera and light. This procedure is designed to examine the lower third of the colon, specifically the sigmoid colon and rectum. Colonoscopy, on the other hand, uses a longer instrument called a colonoscope, allowing for a comprehensive examination of the entire colon, from the rectum to the cecum.
Screening intervals vary based on the procedure. Colonoscopy is typically recommended every 10 years for average-risk individuals, given its extensive scope and thoroughness. In contrast, sigmoidoscopy is usually suggested every 5 years, as it focuses on a more limited section of the colon. In terms of patient experience, sigmoidoscopy is less invasive and generally does not require sedation, making it a more straightforward procedure for many patients.10Jodal, H. C., Helsingen, L. M., Anderson, J. C., Lytvyn, L., Vandvik, P. O., & Emilsson, L. (2019). Colorectal cancer screening with fecal testing, sigmoidoscopy or colonoscopy: a systematic review and network meta-analysis. BMJ open, 9(10), e032773.
While colonoscopy is the preferred screening method for comprehensive evaluations, sigmoidoscopy may be favored in specific situations, such as for patients unable to tolerate sedation or requiring a targeted examination of the lower colon. Both procedures are valuable tools in colorectal cancer prevention and should be chosen based on individual risk factors, medical history, and patient preferences.11Juul, F. E., Cross, A. J., Schoen, R. E., Senore, C., Pinsky, P. F., Miller, E. A., … & Løberg, M. (2024). Effectiveness of Colonoscopy Screening vs Sigmoidoscopy Screening in Colorectal Cancer. JAMA Network Open, 7(2), e240007-e240007.
Final Remarks
Sigmoidoscopy is an essential screening tool for colorectal health diagnosis and screening. The ability of sigmoidoscopy to provide direct visualization of the lower makes it more invaluable for early detection of colorectal cancer. Abnormal findings of this test can provide critical insights into various other gastrointestinal disorders, enabling timely diagnosis and management of the condition.
Refrences
- 1Winawer, S. J., Miller, C., Lightdale, C., Herbert, E., Ephram, R. C., Gordon, L., & Miller, D. (1987). Patient response to sigmoidoscopy: a randomized, controlled trial of rigid and flexible sigmoidoscopy. Cancer, 60(8), 1905-1908.
- 2Harper, M. B., & Pope, J. B. (1997). Flexible sigmoidoscopy. Primary Care: Clinics in Office Practice, 24(2), 341-357.
- 3Rao, V. S. R., Ahmad, N., Al‐Mukhtar, A., Stojkovic, S., Moore, P. J., & Ahmad, S. M. (2005). Comparison of rigid vs. flexible sigmoidoscopy in the detection of significant anorectal lesions. Colorectal Disease, 7(1), 61-64.
- 4Simpson, P. J., McMurrick, P. J., Polglase, A. L., & Koh, C. E. (2010). Comparison of equipment management and cleaning protocols for rigid sigmoidoscopy. ANZ Journal of Surgery, 80(10), 728-731.
- 5Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
- 6Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
- 7Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
- 8Zuber, T. J. (2001). Flexible sigmoidoscopy. American Family Physician, 63(7), 1375-1380.
- 9Miller, B. E. Patient preparation for sigmoidoscopy. SIGMOIDOSCOPY AND CYSTOSCOPY, 33.
- 10Jodal, H. C., Helsingen, L. M., Anderson, J. C., Lytvyn, L., Vandvik, P. O., & Emilsson, L. (2019). Colorectal cancer screening with fecal testing, sigmoidoscopy or colonoscopy: a systematic review and network meta-analysis. BMJ open, 9(10), e032773.
- 11Juul, F. E., Cross, A. J., Schoen, R. E., Senore, C., Pinsky, P. F., Miller, E. A., … & Løberg, M. (2024). Effectiveness of Colonoscopy Screening vs Sigmoidoscopy Screening in Colorectal Cancer. JAMA Network Open, 7(2), e240007-e240007.



