Bilateral carpal tunnel syndrome is a clinical condition caused by localized compression of the median nerve at the wrist. It is characterized by numbness, tingling, burning, and pain affecting the fingers and palm, particularly in the areas supplied by the median nerve.
Carpal tunnel syndrome (CTS) is the most common type of compression neuropathy, where prolonged nerve compression leads to sensory disturbances and motor weakness. Patients often experience numbness, tingling sensations, and pain in the thumb, index, middle, and radial half of the ring finger. Some individuals may also notice hand weakness and thenar muscle atrophy, which can impair hand function and fine motor skills.
Carpal Tunnel syndrome
Carpal tunnel syndrome (CTS) is a common condition characterized by tingling, numbness, and hand weakness. It develops when the median nerve, which runs through the wrist, is subjected to increased pressure within the carpal tunnel. The median nerve provides sensation to the thumb, index finger, middle finger, and thumb side of the ring finger. Typically, the little finger (“pinky”) remains unaffected, as it is supplied by the ulnar nerve.
CTS is the most common upper extremity compressive neuropathy, affecting an estimated 1 to 5 percent of the general population.1Werner RA, Andary M. Carpal tunnel syndrome: Clinical manifestations and diagnosis. UpToDate. Available at: https://www.uptodate.com/contents/carpal-tunnel-syndrome-clinical-manifestations-and-diagnosis. Accessed April 26, 2025. It is notably more common in women, with females being affected about three times more often than males. Over time, affected individuals may experience clumsiness in hand movements and a progressive loss of pinch and grip strength.2Dec, P., & Zyluk, A. (2018). Bilateral carpal tunnel syndrome – A review. Neurologia i neurochirurgia polska, 52(1), 79–83. https://doi.org/10.1016/j.pjnns.2017.09.009
What is Carpal Tunnel?
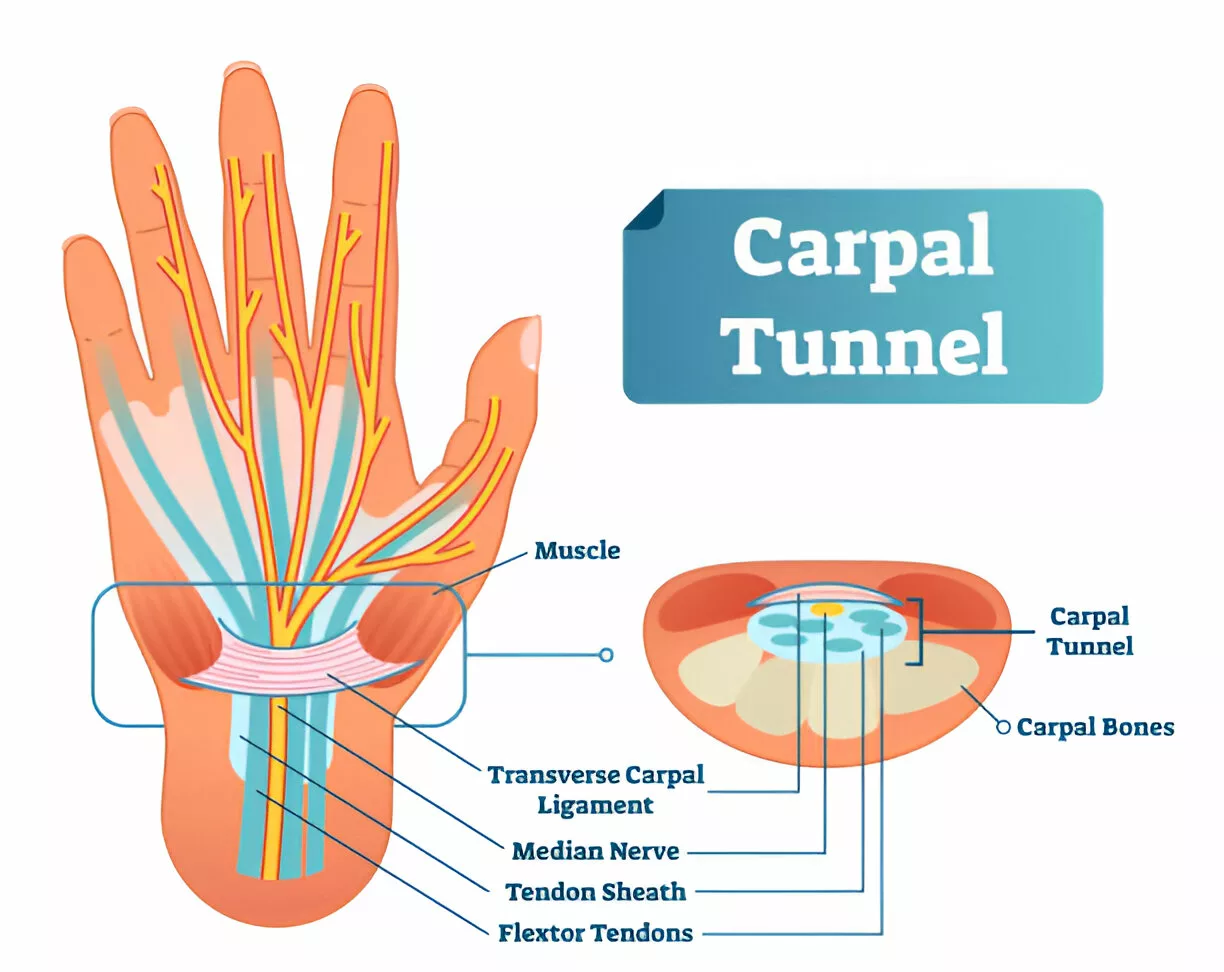
The carpal tunnel is the space in the wrist that holds tendons and the median nerve. This tunnel’s components are as follows:
- Bones: The sides and bottom of the tunnel are made up of carpal bones. They have a semi-circular shape.
- Ligament: The roof of the tunnel is formed by a strong connective tissue called the transverse carpal ligament.
- Tendons: Tendons, which resemble rope-like structures, link the forearm’s muscles to the hand’s bones. They permit the thumb and fingers to flex.
Tendons and the median nerve are located inside the tunnel. Most of the digits, except the little finger, receive sensations from the median nerve. Additionally, it strengthens the thumb and index finger bases.
Symptoms of Bilateral Carpal Tunnel Syndrome
Bilateral carpal tunnel syndrome (CTS) commonly presents with sensory symptoms affecting the areas supplied by the median nerve, including the thumb, index finger, middle finger, and the radial side of the ring finger. Symptoms may include:3Carpal tunnel syndrome. Mayo Clinic. Available at: https://www.mayoclinic.org/diseases-conditions/carpal-tunnel-syndrome/symptoms-causes/syc-20355603. Accessed April 26, 2025.
- Numbness and tingling in the median-innervated fingers
- Pain that may be localized to the wrist, spread across the entire hand, or occasionally radiate up the forearm and, less commonly, to the shoulder
- Burning sensations or discomfort, especially during activities requiring wrist flexion or extension (such as typing, driving, or holding a book)
- Nighttime symptoms that may awaken the patient, often relieved temporarily by shaking or wringing the hands
In more advanced or severe cases, additional symptoms may develop:
- Hand weakness or clumsiness, leading to difficulty with tasks like gripping objects, turning keys, buttoning clothing, or opening jars
- Atrophy of the thenar muscles (muscle wasting at the base of the thumb)
- Progression from intermittent sensory complaints to persistent sensory loss, while sparing the thenar eminence due to the anatomical course of the palmar cutaneous branch
Bilateral CTS is relatively common, reported in up to 65% of patients.4StatPearls. (2025). Carpal tunnel syndrome. Retrieved April 26, 2025, from https://www.ncbi.nlm.nih.gov/books/NBK448179/ However, it often starts asymmetrically, with one hand being more noticeably symptomatic at first.
What Causes Carpal Tunnel Syndrome (CTS)?
The exact cause of Carpal Tunnel Syndrome (CTS) is not fully understood, but several factors are believed to contribute to the increased pressure on the median nerve within the carpal tunnel. These include:5Bland JD. Carpal tunnel syndrome. Curr Opin Neurol. 2005 Oct;18(5):581-5. doi: 10.1097/01.wco.0000173142.58068.5a. PMID: 16155444.
- Anatomic Compression: Compression may result from swelling of the flexor tendons, fibrosis, or space-occupying lesions like cysts. Conditions such as rheumatoid arthritis or a congenitally small carpal tunnel can also contribute.6Amirfeyz R, Gozzard C, Leslie IJ. Hand elevation test for assessment of carpal tunnel syndrome. J Hand Surg Br. 2005 Aug;30(4):361-4. doi: 10.1016/j.jhsb.2005.04.007. PMID: 15951075.
- Inflammation: Chronic pressure can lead to inflammation, causing swelling and thickening of the nerve and surrounding tissues. This inflammation may damage the nerve over time.
Posture plays a role as well—wrist flexion or extension can increase pressure within the carpal tunnel, potentially exacerbating symptoms.
Tests for Diagnosis of Bilateral Carpal Tunnel Syndrome
Diagnosis begins with a careful clinical examination, followed by specific tests to evaluate the function of the median nerve and confirm carpal tunnel syndrome.
Tinel’s Sign:
During Tinel’s test, the doctor gently taps over the median nerve at the wrist. If the patient experiences tingling, a mild electric shock sensation, or numbness in the fingers (particularly the thumb, index, and middle fingers), the test is considered positive and may suggest carpal tunnel syndrome (CTS).
Phalen’s Maneuver:
Also known as the wrist-flexion test, this maneuver involves the patient pressing the backs of their hands and fingers together with wrists fully flexed (pointed downward at a 90-degree angle) and holding the position for about 30 to 60 seconds. A positive test occurs when tingling or numbness develops in the distribution of the median nerve.
The Two-Point Discrimination Test:
In this sensory test, a device called a two-point discriminator is used to assess the ability to distinguish two closely spaced points on the skin. In carpal tunnel syndrome, the ability to distinguish between two points may be reduced due to sensory nerve impairment.
Electromyogram (E.M.G.) & Nerve Conduction Velocity Test:
An EMG measures the electrical activity of muscles, while a nerve conduction study evaluates how fast electrical impulses move through the median nerve. Small electrodes are placed on the skin, and mild electrical stimulation is used to assess nerve function. These tests are valuable in confirming the diagnosis and ruling out other conditions that mimic CTS.7Rosario NB, De Jesus O. Electrodiagnostic Evaluation of Carpal Tunnel Syndrome. [Updated 2023 Aug 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562235/
X-rays:
Although X-rays do not diagnose carpal tunnel syndrome directly, they are useful to exclude other conditions, such as wrist fractures, arthritis, or bone abnormalities, that could be contributing to the patient’s symptoms.
Management of Bilateral Carpal Tunnel Syndrome
Carpal tunnel syndrome (CTS) is often managed initially with nonsurgical interventions aimed at relieving pain and reducing inflammation. The goal of these treatments is to alleviate symptoms and prevent progression to more severe cases.
Non-Surgical Treatments
Medications:
- Non-steroidal anti-inflammatory drugs (NSAIDs) are the first choice to treat CTS conservatively. These drugs alleviate pain and swelling.
- In some cases, oral corticosteroids or corticosteroid injections into the carpal tunnel may be used to provide more targeted, short-term relief from inflammation.
- Vitamin B6 supplements (pyridoxine) have been suggested as a treatment option, though high doses should be avoided as they can cause nerve problems (neuropathy).
Conservative Therapy Approach:
A well-rounded conservative approach can include a combination of the following strategies, often summarized as B.R.E.M — Brace, Rest, Exercise, and Massage.
Brace
Wearing a wrist brace, especially at night, helps prevent movements that could worsen the condition. It is crucial to use a certified carpal tunnel brace designed specifically for CTS, as general braces may exacerbate symptoms. Additionally, avoid wearing the brace during activities that could stress the tendons further.8Stanek, E. J., 3rd, & Pransky, G. (1996). Unilateral vs. bilateral carpal tunnel: challenges and approaches. American journal of industrial medicine, 29(6), 669–678. https://doi.org/10.1002/(SICI)1097-0274(199606)29:6<669::AID-AJIM11>3.0.CO;2-Y
Rest
Rest is key to allowing the affected area to heal. Refrain from activities that contributed to the development of CTS, such as repetitive hand movements at work. This is especially relevant for individuals in occupations that require extensive hand use.
Exercise
Regular stretching exercises, such as stretching the fingers for 30 seconds after every 30 minutes of work, can help prevent tendon strain and promote better circulation. These “mini-breaks” are essential to maintaining hand flexibility and reducing the risk of further injury.
Massage
Myofascial release massage techniques have been shown to reduce inflammation and improve blood flow in the wrist. Proper technique is essential for these massages to be effective, particularly for CTS or wrist tendonitis.9Sucher BM. Myofascial release of carpal tunnel syndrome. J Am Osteopath Assoc. 1993 Jan;93(1):92-4, 100-1. PMID: 8423131.
Surgical Treatment
Surgical intervention is often required for patients with moderate to severe Carpal Tunnel Syndrome (CTS) who do not respond to conservative measures or for those who experience persistent symptoms such as muscle weakness, atrophy, or numbness. The following surgical options are available:
Open Carpal Tunnel Release (OCTR):
In this traditional procedure, a longitudinal incision (approximately 2 inches) is made over the wrist, and the transverse carpal ligament is surgically divided to relieve pressure on the median nerve. This approach provides direct access to the carpal tunnel, ensuring thorough release of the ligament. The recovery time is typically longer, and the procedure carries a slightly higher risk of complications, such as infection and nerve injury. However, it remains the most widely used technique, particularly in severe cases.
Endoscopic Carpal Tunnel Release (ECTR):
ECTR is a minimally invasive technique that utilizes small incisions and a small camera (endoscope) to guide the division of the transverse carpal ligament. This approach is associated with faster recovery and less postoperative pain compared to OCTR. However, the risk of transient nerve injury may be slightly higher in ECTR due to the limited visibility and smaller incisions. Despite this, ECTR has become a preferred choice for many surgeons in suitable patients, especially those with mild to moderate CTS.
Postoperative Care and Recovery
After either surgical procedure, patients are typically given local anesthesia, and the wrist is wrapped in a thick bandage to promote healing and limit movement. In normal scenerios, the recovery time is up to six weeks, during which patients are advised to avoid heavy lifting and wrist strain. Additionally, occupational therapy may be recommended to aid in recovery, particularly in regaining wrist mobility and strength.
Surgical outcomes are generally favorable, with success rates for CTS release ranging from 85% to 95%.10Lusa V, Karjalainen TV, Pääkkönen M, Rajamäki TJ, Jaatinen K. Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev. 2024 Jan 8;1(1):CD001552. doi: 10.1002/14651858.CD001552.pub3. PMID: 38189479; PMCID: PMC10772978. While recurrence of symptoms is rare, long-term follow-up is important to monitor for any potential complications.
Differential Diagnoses
If you have pain or numbness in your fingers, hands, or wrists, the most important thing is to determine its cause. There are other sets of reasons that cause the same pain. The most common disorder than can mimic CTS is cervical radiculopathy.
Cervical Radiculopathy:
This condition, particularly involving the C6 or C7 nerve roots, can mimic CTS, causing arm pain and paresthesia. Key features that suggest cervical radiculopathy include neck pain radiating into the shoulder and arm, exacerbation of symptoms with neck movement, and reduced reflexes in the upper limbs. Motor dysfunction and sensory loss in the forearm or medial palm can also occur.11UpToDate. (2025). Cervical radiculopathy: Clinical features and diagnosis. Retrieved April 26, 2025, from https://www.uptodate.com/contents/cervical-radiculopathy-clinical-features-and-diagnosis
Other conditions inlcude:
- De Quervain’s Tenosynovitis: This condition involves inflammation of the tendons at the base of the thumb, causing pain, particularly when making a fist or moving the thumb. It is often aggravated by actions such as shaking hands.
- Trigger Finger: Trigger finger (or stenosing tenosynovitis) is characterized by pain and stiffness at the base of the finger or thumb. The affected digit may become locked in a bent position or “catch” when straightening.
- Arthritis: A condition affecting the joints, which can cause pain, swelling, and stiffness. It can lead to gradual joint degeneration. Osteoarthritis is the most common type of degenerative arthritis, but other types, like rheumatoid arthritis, can also affect the hand and wrist joints.
- Acute Calcific Tendonitis — Acute calcific tendonitis (ACT) is a rare idiopathic inflammatory disorder that usually affects the small joints and tendons of the upper limb. While it commonly involves the shoulder, it can occasionally affect the wrist and mimic the symptoms of Carpal Tunnel Syndrome. Due to its rarity and clinical similarity to infections or inflammatory conditions, ACT is frequently misdiagnosed. Symptomatic management with NSAIDs typically resolves symptoms within a week.12Lee, Y. J., Lee, S. H., & Choi, S. H. (2011). Acute calcific tendinitis of the hand and wrist: a report of 12 cases and literature review. Journal of Hand Surgery (European Volume), 36(5), 398–403. https://doi.org/10.1177/1753193410392239
Take Home Message
Wrist tendinitis frequently receives the incorrect diagnosis of carpal tunnel syndrome. On the other hand, wrist tendinitis is commonly misdiagnosed as carpal tunnel syndrome. Nevertheless, regardless of the diagnosis, you can take action to lessen the symptoms of either illness. Furthermore, it’s important to act quickly before symptoms get worse.
Refrences
- 1Werner RA, Andary M. Carpal tunnel syndrome: Clinical manifestations and diagnosis. UpToDate. Available at: https://www.uptodate.com/contents/carpal-tunnel-syndrome-clinical-manifestations-and-diagnosis. Accessed April 26, 2025.
- 2Dec, P., & Zyluk, A. (2018). Bilateral carpal tunnel syndrome – A review. Neurologia i neurochirurgia polska, 52(1), 79–83. https://doi.org/10.1016/j.pjnns.2017.09.009
- 3Carpal tunnel syndrome. Mayo Clinic. Available at: https://www.mayoclinic.org/diseases-conditions/carpal-tunnel-syndrome/symptoms-causes/syc-20355603. Accessed April 26, 2025.
- 4StatPearls. (2025). Carpal tunnel syndrome. Retrieved April 26, 2025, from https://www.ncbi.nlm.nih.gov/books/NBK448179/
- 5Bland JD. Carpal tunnel syndrome. Curr Opin Neurol. 2005 Oct;18(5):581-5. doi: 10.1097/01.wco.0000173142.58068.5a. PMID: 16155444.
- 6Amirfeyz R, Gozzard C, Leslie IJ. Hand elevation test for assessment of carpal tunnel syndrome. J Hand Surg Br. 2005 Aug;30(4):361-4. doi: 10.1016/j.jhsb.2005.04.007. PMID: 15951075.
- 7Rosario NB, De Jesus O. Electrodiagnostic Evaluation of Carpal Tunnel Syndrome. [Updated 2023 Aug 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562235/
- 8Stanek, E. J., 3rd, & Pransky, G. (1996). Unilateral vs. bilateral carpal tunnel: challenges and approaches. American journal of industrial medicine, 29(6), 669–678. https://doi.org/10.1002/(SICI)1097-0274(199606)29:6<669::AID-AJIM11>3.0.CO;2-Y
- 9Sucher BM. Myofascial release of carpal tunnel syndrome. J Am Osteopath Assoc. 1993 Jan;93(1):92-4, 100-1. PMID: 8423131.
- 10Lusa V, Karjalainen TV, Pääkkönen M, Rajamäki TJ, Jaatinen K. Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev. 2024 Jan 8;1(1):CD001552. doi: 10.1002/14651858.CD001552.pub3. PMID: 38189479; PMCID: PMC10772978.
- 11UpToDate. (2025). Cervical radiculopathy: Clinical features and diagnosis. Retrieved April 26, 2025, from https://www.uptodate.com/contents/cervical-radiculopathy-clinical-features-and-diagnosis
- 12Lee, Y. J., Lee, S. H., & Choi, S. H. (2011). Acute calcific tendinitis of the hand and wrist: a report of 12 cases and literature review. Journal of Hand Surgery (European Volume), 36(5), 398–403. https://doi.org/10.1177/1753193410392239
