
Alveolar ridge augmentation, or ridge augmentation, is a dental procedure done to recontour the jaw and gums to achieve a more natural shape. Tooth extraction and/or bone loss potentially leads to reshaping of the alveolar bone, which causes bone shrinkage on the extraction site. A lot of the time, designing a prosthesis over the shrunken, deteriorated alveolar ridge is unfeasible. So, doctors augment the bone for better prostheses like complete dentures and dental implants. In modern times, professionals frequently perform ridge augmentation procedures before placing dental implants.
The most common techniques of augmenting bone include horizontal and vertical techniques. Doctors usually choose from different graft materials (bone substitutes), including autografts (the patient’s own bone graft), allografts (bone graft from a donor), or alloplasts (synthetic bone materials). It is a technique-sensitive procedure, so surgeons try to be extra cautious and minimize complications.1Kim, Y. K., & Ku, J. K. (2020). Ridge augmentation in implant dentistry. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 46(3), 211-217.
What is the Alveolar Ridge?
The alveolar ridge refers to the part of the jawbone that houses the teeth (surrounds the tooth roots). When the doctor extracts your tooth (due to pulpal necrosis or other reasons) or you lose a tooth (in case of trauma/injury), an open socket is left behind. The open socket heals on its own, and the body covers it with bone and tissue. However, during the healing process, the alveolar bone loses its original height and width.
It was found in a study that the clinical loss in width (3.87mm) is greater than the loss in height (1.53mm).2Van der Weijden, F., Dell’Acqua, F., & Slot, D. E. (2009). Alveolar bone dimensional changes of post‐extraction sockets in humans: a systematic review. Journal of clinical periodontology, 36(12), 1048-1058. Furthermore, the width and height of the socket continue to deteriorate over time as there is no stimulation of bone maintenance from a tooth.
What Causes Jaw Bone Deterioration?
A depressed ridge is unsuitable for prosthesis success. There are multiple reasons that can lead to a deteriorated alveolar ridge, including:
- Extraction
- Injury/trauma
- Periodontitis
- Long-term use of dentures
- Birth/congenital defects
So, to ensure a robust, well-retained, and aesthetically pleasing tooth replacement, most dentists opt for a ridge augmentation before planning a prosthesis.
Ridge Augmentation Preparation
Radiographic Analysis:
Before starting the procedure, your dentist might order multiple X-rays to study the bone dimensions. Orthopantogram (OPG) X-rays, i.e., panoramic dental X-rays, play a crucial role in bone assessment for augmentation procedures. The doctor may also take your mouth impression and make a pre-operative cast to compare the results. Modern clinics take 3D scans of your oral structures and face to devise a customized treatment plan.
Anesthesia:
It’s an in-office procedure where most dentists prefer to give local anesthesia (LA). However, if available, you can request to get it done under conscious sedation, which involves inhaling nitrous oxide gas, or you can go for intravenous sedation (IV sedation).
Ridge Augmentation Techniques
Your doctor decides which technique of augmentation will work best during the pre-operative workup. The dentist will opt for either horizontal or vertical ridge augmentation after the anesthesia has set in.
Vertical Vs. Horizontal Ridge Augmentation
When the aim is to increase the width of the alveolar ridge, your doctor will choose the horizontal ridge technique, and when an increase in ridge height is the primary purpose, professionals opt for vertical ridge augmentation.
Horizontal ridge augmentation is the more frequently adopted procedure and is an effective way for rehabilitation in fully and partially edentulous patients. The procedure is commonly done in the mandible. It is completely safe and maximizes implant survival and success.3Smeets, R., Matthies, L., Windisch, P., Gosau, M., Jung, R., Brodala, N., … & Knipfer, C. (2022). Horizontal augmentation techniques in the mandible: a systematic review. International journal of implant dentistry, 8(1), 23. Ridge augmentation and dental implant placement can be done at the same time (simultaneous approach) or performed in two stages (staged approach).
Vertical augmentation is done in cases with extensive bone loss. With enhanced height of the alveolar ridge, doctors can safely place implants away from crucial structures like the inferior alveolar nerve (which is challenging!). This overcomes the need for tilted and shorter implants.4Urban, I. A., Montero, E., Amerio, E., Palombo, D., & Monje, A. (2023). Techniques on vertical ridge augmentation: Indications and effectiveness. Periodontology 2000, 93(1), 153-182.
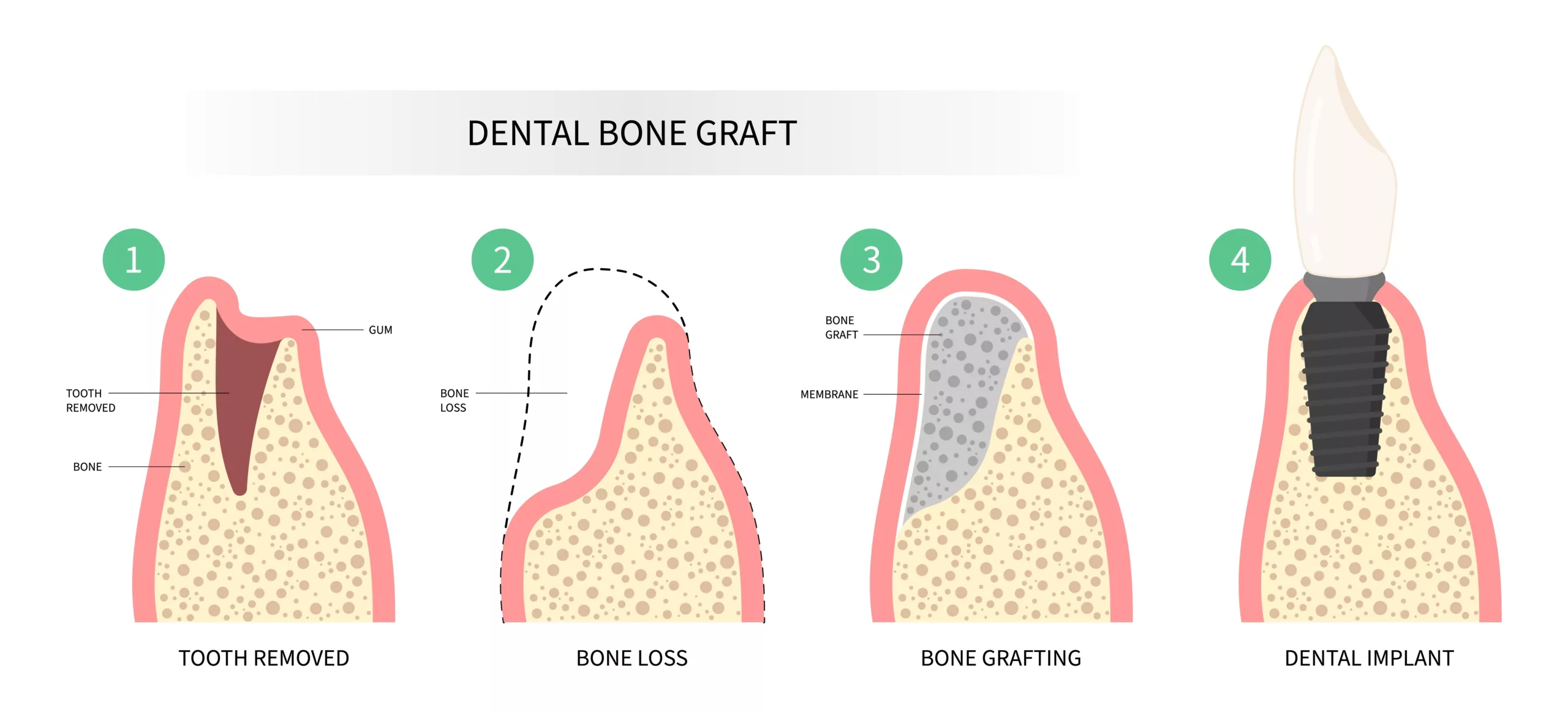
How Is Ridge Augmentation Performed?
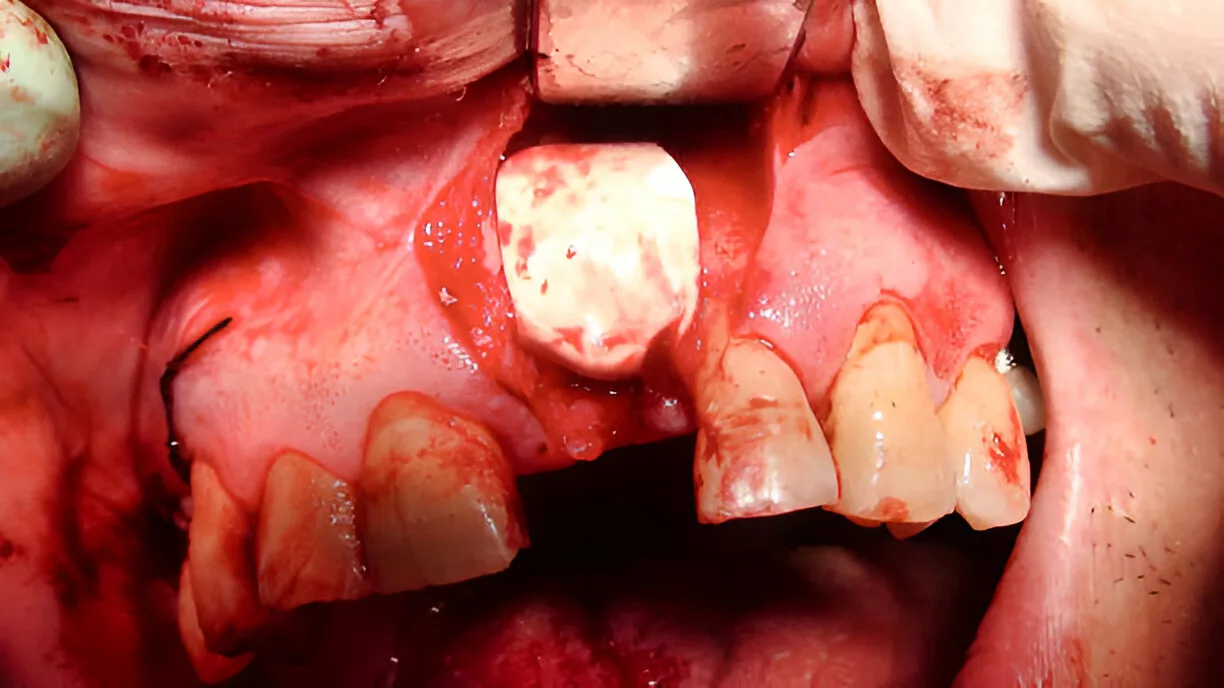
After anesthesia, the doctor makes an incision in the gingiva (gum) and exposes the bone (area of focus). Ridge augmentation is mostly done right after a tooth extraction. However, sometimes, doctors perform augmentation after implant placement.
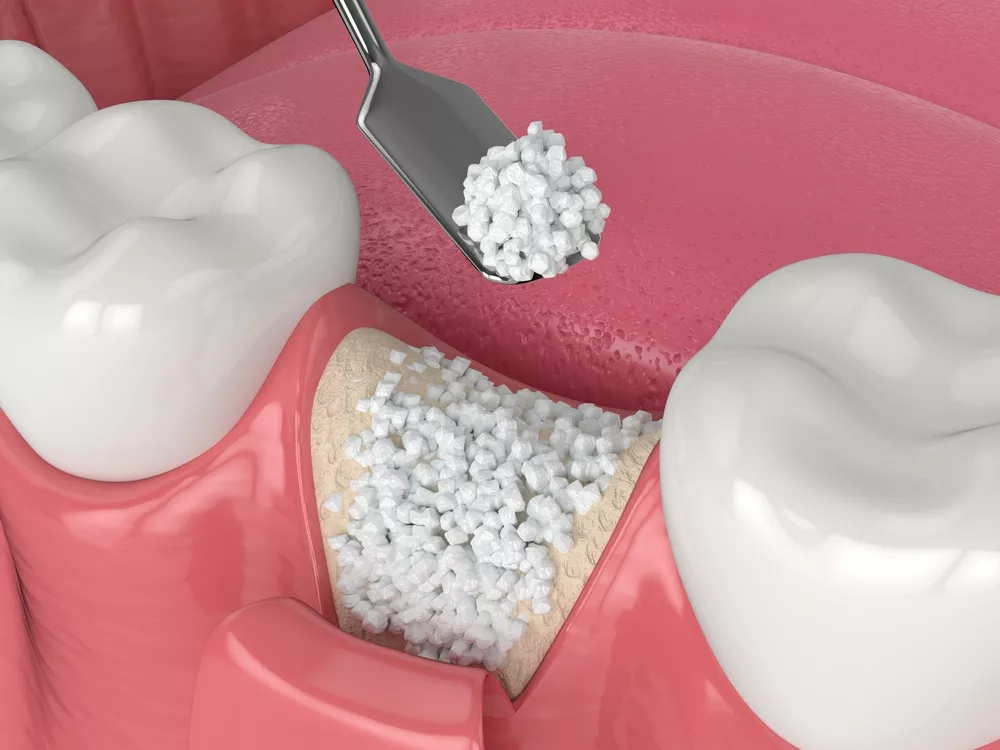
The graft material is placed in the tooth socket to prevent loss of ridge dimensions. When performed later (sometime after tooth extraction), the surgeon places the bone graft on the exposed bone surface.
Types Of Bone Grafts:
Common types of bone graft include:
Autograft
An autogenous bone graft refers to bone taken from another part of the patient’s body. The iliac crest of the hip is the most common donor site for an autograft. However, your doctor can take a graft from the chin or the back of the lower jaw. Autogenous grafts cause bone generation by osteogenesis, i.e., formation of new bone from undifferentiated cells.
Studies show that grafts from the mandibular symphysis show excellent results in maxillary ridge augmentation when used with platelet-rich fibrin.5Paul, N., Jyotsna, S., & Keshini, M. P. (2022). Alveolar ridge augmentation using autogenous bone graft and platelet-rich fibrin to facilitate implant placement. Contemporary Clinical Dentistry, 13(1), 90-94. In the current scenario, autogenous graft is considered the “gold standard” due to faster healing time and better tissue acceptance.
Allograft
This type of bone graft is taken from deceased donors (who have donated to bone banks). Allografts are generally not preferred because there is a risk of tissue/organ rejection. One study concluded that all grafts provided similar implant success.6Chavda, S., & Levin, L. (2018). Human studies of vertical and horizontal alveolar ridge augmentation comparing different types of bone graft materials: a systematic review. Journal of Oral Implantology, 44(1), 74-84.
Allografts promote bone formation by osteoconduction, i.e., new bone deposition (from undifferentiated cells) is encouraged by a physical matrix (or a bio-inert scaffold) and osteoinduction, i.e., transformation of undifferentiated cells into bone-forming cells (osteoblasts) through growth factors found in the living bone. Another clinical study demonstrated that the use of allografts was associated with complications like increased discomfort and morbidity, which limits their acceptance by the patient.7Peck, M. T. (2015). Alveolar ridge augmentation using the allograft bone shell technique. J Contemp Dent Pract, 16(9), 768-773.
Xenograft
A xenogenous graft is a processed mineral component derived from a bone graft taken from an animal (cow or pig, etc.). Xenogenous grafts serve to be feasible alternatives to autogenous bone grafts in horizontal ridge augmentation.8 Azambuja Carvalho, P. H., dos Santos Trento, G., Moura, L. B., Cunha, G., Gabrielli, M. A. C., & Pereira-Filho, V. A. (2019). Horizontal ridge augmentation using xenogenous bone graft—systematic review. Oral and maxillofacial surgery, 23, 271-279. Xenografts induce bone formation primarily by osteoconduction.
Alloplast
This type of bone graft accelerates the process of bone formation (on the desired site) and is mostly synthetic (man-made). The graft may contain minerals derived from natural sources. With alloplasts, there are minimal chances of infection and disease.
After placing the bone graft, the surgeon carefully stitches (closes) the incision. New bone tissue forms over the ridge in the next few months. However, nowadays, doctors prefer speeding up the healing process by covering the graft with a membrane, a process called guided tissue regeneration (GTR).
Ridge Augmentation With Guided Tissue Regeneration (GTR)
In guided tissue regeneration, your doctor will place a specialized barrier membrane over the grafted bone tissue. After placing the barrier in place, the surgeon stitches the gum back. The main aim of GTR is to speed up the process of bone healing. Doctors across the globe use different types of membrane materials to achieve superior bone healing in ridge augmentation. Surgeons most frequently use biodegradable collagen membrane in horizontal bone augmentation surgeries, whereas bioinert polytetrafluoroethylene (PTFE) is the material of choice for vertical augmentation.9Buser, D., Urban, I., Monje, A., Kunrath, M. F., & Dahlin, C. (2023). Guided bone regeneration in implant dentistry: Basic principle, progress over 35 years, and recent research activities. Periodontology 2000, 93(1), 9-25.
Guided bone regeneration (GBR) is a safe and predictable treatment, but there are several complications associated with this procedure. The cross-linked collagen membranes tend to cause adverse effects like infection, tissue dehiscence, and bone exposure. In some cases, these effects undermine the efficacy of GTR.10Calciolari, E., Corbella, S., Gkranias, N., Viganó, M., Sculean, A., & Donos, N. (2023). Efficacy of biomaterials for lateral bone augmentation performed with guided bone regeneration. A network meta‐analysis. Periodontology 2000, 93(1), 77-106.
Ridge Augmentation Healing Time
The healing time for ridge augmentation varies between individuals. It depends on multiple factors, such as the size and type of the graft material and patient factors (such as age and presence of comorbidities, etc.). It generally takes 4-12 months to reach the desired results. For autogenous bone, the healing time is 4-6 months, while for procedures without autogenous graft, it is at least 12 months.
What To Do After Ridge Augmentation?
- Take the prescribed medications regularly.
- Try to chew on the opposite side of the mouth to avoid post-operative complications.
- Apply an ice pack (or a frozen bag of vegetables) to the surgical site to minimize swelling quickly. Do this in 20-minute sessions for the first 24-48 hours after surgery.
- Try to keep your head elevated while sleeping.
- Be sure to wear the appliance/denture, if provided by the dentist.
- If the dentist has placed a surgical dressing, try to keep it in position till the next appointment.
- Avoid smoking and drinking for a week (at least) to allow uneventful healing.
Ridge Augmentation Vs. Bone Graft
Bone grafting is a surgical technique used to help new bone grow after a tooth is lost or damaged. It involves placing bone material into the area to stimulate natural bone healing and regeneration. Bone grafting can be done for different reasons, such as preserving the socket after a tooth extraction, preparing for a dental implant, or strengthening weak areas of the jawbone. Ridge augmentation is a specific type of bone grafting procedure that focuses on rebuilding and reshaping the jawbone, also called the alveolar ridge. This is often needed when the bone has shrunk after tooth loss and needs to be restored for esthetic reasons or to support dental implants properly. Ridge augmentation is different from a gum graft, which is a procedure used to treat gum recession.
Wrapping Up
Ridge augmentation is the process of reshaping and rebuilding the alveolar ridge for aesthetic purposes or prosthesis (implants). Dentists perform horizontal or vertical ridge augmentation to increase the width or height of the bone, respectively, for successful implant placement. Mostly done under local anesthesia, doctors place bone grafts at the shrunken site to add volume to the region. Different types of grafts, i.e., autografts (from the patient), allografts (from human donors), xenografts (from pigs/cows), alloplasts (synthetic), can be used. Nowadays, doctors place a barrier membrane (collagen membrane or bioinert PTFE) over the newly added bone to speed up the healing process. Complete revamping of the bone takes 4-12 months. You have to follow post-operative care for about 2 weeks.
Refrences
- 1Kim, Y. K., & Ku, J. K. (2020). Ridge augmentation in implant dentistry. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 46(3), 211-217.
- 2Van der Weijden, F., Dell’Acqua, F., & Slot, D. E. (2009). Alveolar bone dimensional changes of post‐extraction sockets in humans: a systematic review. Journal of clinical periodontology, 36(12), 1048-1058.
- 3Smeets, R., Matthies, L., Windisch, P., Gosau, M., Jung, R., Brodala, N., … & Knipfer, C. (2022). Horizontal augmentation techniques in the mandible: a systematic review. International journal of implant dentistry, 8(1), 23.
- 4Urban, I. A., Montero, E., Amerio, E., Palombo, D., & Monje, A. (2023). Techniques on vertical ridge augmentation: Indications and effectiveness. Periodontology 2000, 93(1), 153-182.
- 5Paul, N., Jyotsna, S., & Keshini, M. P. (2022). Alveolar ridge augmentation using autogenous bone graft and platelet-rich fibrin to facilitate implant placement. Contemporary Clinical Dentistry, 13(1), 90-94.
- 6Chavda, S., & Levin, L. (2018). Human studies of vertical and horizontal alveolar ridge augmentation comparing different types of bone graft materials: a systematic review. Journal of Oral Implantology, 44(1), 74-84.
- 7Peck, M. T. (2015). Alveolar ridge augmentation using the allograft bone shell technique. J Contemp Dent Pract, 16(9), 768-773.
- 8Azambuja Carvalho, P. H., dos Santos Trento, G., Moura, L. B., Cunha, G., Gabrielli, M. A. C., & Pereira-Filho, V. A. (2019). Horizontal ridge augmentation using xenogenous bone graft—systematic review. Oral and maxillofacial surgery, 23, 271-279.
- 9Buser, D., Urban, I., Monje, A., Kunrath, M. F., & Dahlin, C. (2023). Guided bone regeneration in implant dentistry: Basic principle, progress over 35 years, and recent research activities. Periodontology 2000, 93(1), 9-25.
- 10Calciolari, E., Corbella, S., Gkranias, N., Viganó, M., Sculean, A., & Donos, N. (2023). Efficacy of biomaterials for lateral bone augmentation performed with guided bone regeneration. A network meta‐analysis. Periodontology 2000, 93(1), 77-106.



