
What are Rickets?
Rickets is defined as faulty mineralization of growing bone that may be due to vitamin D, calcium, or phosphorus deficiency. When mature bones fail to mineralize, the condition is referred to as osteomalacia. Rickets is a metabolic bone disorder that often results from inadequate vitamin D intake or insufficient sunlight exposure, both of which are essential for calcium absorption and bone health. The most affected age group is children of age 0-2 years.1Gentile, C., & Chiarelli, F. (2021). Rickets in children: An update. Biomedicines, 9(7), 738.https://doi.org/10.3390/biomedicines9070738

Research suggests that an infant requires about 30 minutes of weekly full-body sunlight exposure or two hours of weekly sunlight exposure to the head to maintain adequate vitamin D levels. The most frequent cause of nutritional rickets is a deficiency of vitamin D.2A, B. A., Dahash, & Sankararaman, S. (n.d.). Rickets – statpearls – NCBI bookshelf. Retrieved March 27, 2023, from https://www.ncbi.nlm.nih.gov/books/NBK562285/
Pathology of Rickets
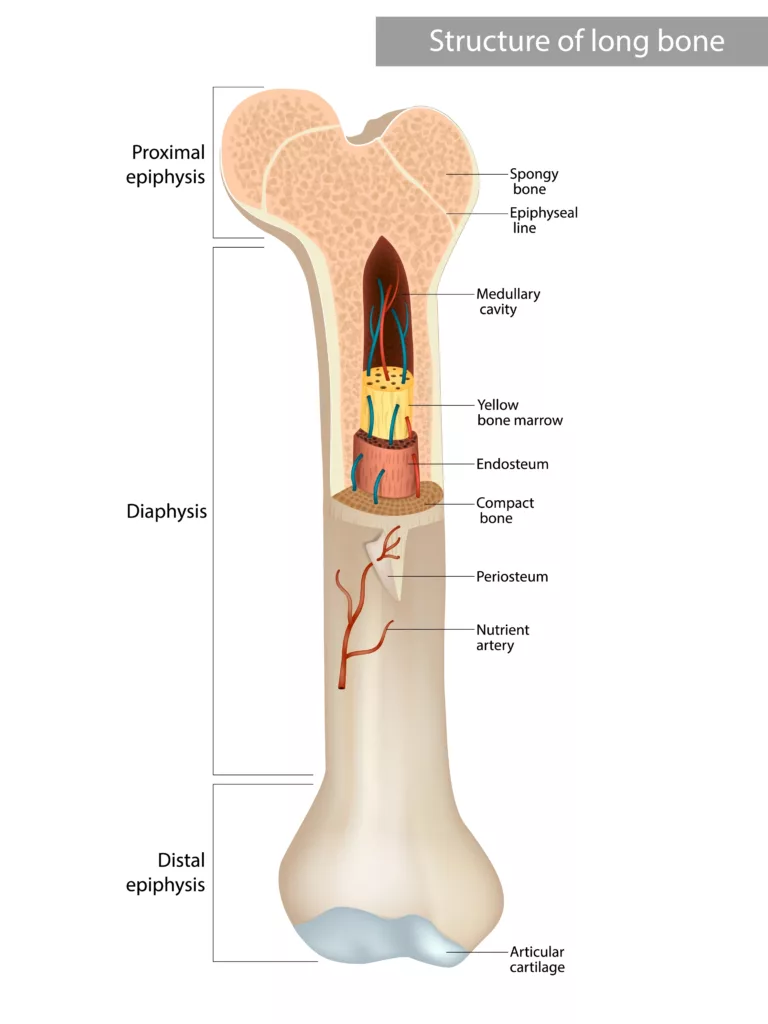
Rickets is characterized by defective bone growth due to inadequate calcification of the epiphyseal cartilage caused by insufficient calcium and phosphorus. This leads to impaired mineralization, with continued growth at the epiphyseal plate resulting in thickening and expansion of the epiphyseal ends, often evident as widened wrists and ankles. Over time, the irregular and weak epiphyseal plates exhibit cupping and fraying, making the bones more prone to fractures. Additionally, the overall softening of bones leads to deformities such as bowed legs, knocked knees, and compression of the skull bones.3Chapman, T., Sugar, N., Done, S., Marasigan, J., Wambold, N., & Feldman, K. (2010). Fractures in infants and toddlers with it. Pediatric radiology, 40, 1184-1189.
What Causes Rickets?
Vitamin D disorders
Vitamin D deficiency is the primary cause of rickets. It may result from inadequate dietary intake, limited sunlight exposure, congenital vitamin D deficiency, or malabsorption disorders. Without sufficient vitamin D, calcium and phosphorus absorption is impaired, disrupting bone mineralization.4Sahay M, Sahay R. Rickets-vitamin D deficiency and dependency. Indian J Endocrinol Metab. 2012 Mar;16(2):164-76. doi: 10.4103/2230-8210.93732. PMID: 22470851; PMCID: PMC3313732.
Deficiency of Calcium
Calcium deficiency can occur due to low dietary intake, malabsorption, or conditions like prematurity that predispose infants to hypocalcemia. Calcium plays a crucial role in bone mineralization, and its deficiency can lead to rickets.5Lambert AS, Linglart A. Hypocalcaemic and hypophosphatemic rickets. Best Pract Res Clin Endocrinol Metab. 2018 Aug;32(4):455-476. doi: 10.1016/j.beem.2018.05.009. Epub 2018 Jul 4. PMID: 30086869.
Phosphorus deficiency
Though rare, phosphorus deficiency can also cause rickets. It may result from inadequate dietary intake, malabsorption, or prematurity, which predisposes infants to hypophosphatemia and subsequent bone abnormalities.
Rickets: Symptoms and Signs
The following symptoms and signs will be seen in a patient with rickets (from head to toe).
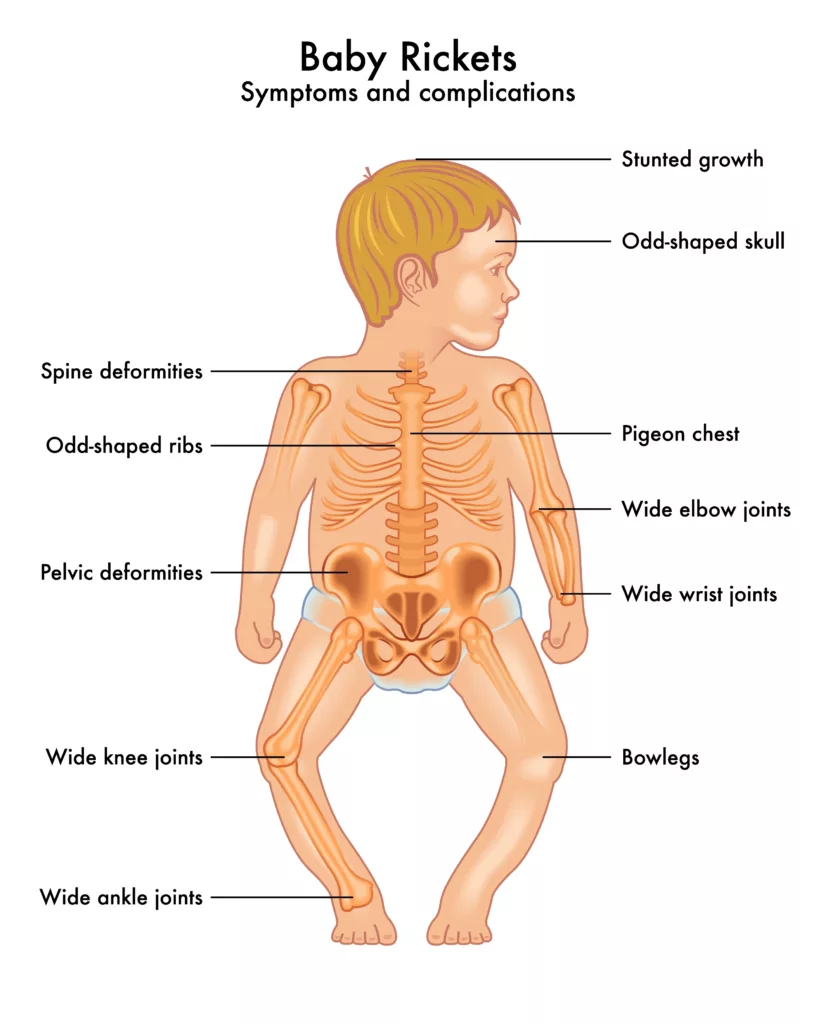
- The head may be larger than normal, or it may be square-like (caput quadratum).
- There may be frontal bossing of the head.
- There will be softening and thinning of skull bones.
- There will be delayed eruption of milk teeth and delayed or defective calcification of permanent teeth.
- Chest deformities, including a pathognomonic “rachitic rosary,” are characterized by bead-like prominences at the costochondral junctions. This can be appreciated on an x-ray chest.6STONE, J. S. DEFORMITIES OF THE CHEST IN RICKETS. Transactions of the American Orthopedic Association s1-11(1):p 337-346, May 1898.
- Harrison’s groove, a horizontal depression along the lower chest
- The ankles and wrists will be widened.
- Bow legs (genu varum) and knock knees (genu valgum) will be appreciated in the lower limbs.
- There will be an Increased chance of greenstick fractures.
How To Diagnose a Case of Rickets?
A history of inadequate vitamin D intake and no exposure to sunlight should alert the physician to go for laboratory tests and X-rays to rule it out.
Laboratory Tests:
Blood tests such as Calcium, phosphorus, and vitamin D levels should be advised. Results will show decreased levels of any one of them or all.
- Serum Calcium: May be decreased
- Serum Phosphorus: Often reduced in phosphorus deficiency
- Alkaline Phosphatase: Elevated due to increased bone turnover
- Vitamin D Levels: Low in vitamin D-related rickets
Imaging Studies:
- X-rays of the Wrist: Characteristic findings include cupping, fraying, and irregularity of the metaphyses.
- Chest X-ray: May show the rachitic rosary in severe cases.
Rickets Treatment
The treatment of rickets varies depending on the specific deficiency. For vitamin D deficiency, doctors prescribe high doses of vitamin D, ranging from 300,000 to 600,000 IU, administered intramuscularly or orally in 2–4 divided doses. Alongside supplementation, ensuring sufficient dietary vitamin D and regular exposure to sunlight is crucial.
Calcium deficiency is managed with oral calcium supplements of at least 500 mg/day, while severe cases may require intravenous calcium. Phosphorus deficiency, though rare, is treated with oral phosphorus supplements (1–3 g/day) combined with vitamin D. A balanced diet rich in vitamin D, calcium, and phosphorus is an integral part of the treatment plan to support healthy bone growth and mineralization.7Biasucci, G., Donini, V., & Cannalire, G. (2024). Rickets Types and Treatment with Vitamin D and Analogues. Nutrients, 16(3), 416. https://doi.org/10.3390/nu16030416
Complications Of Rickets
Following complications may result due to rickets:
- Severe chest deformities can predispose to bronchitis or pneumonia, potentially leading to lung collapse in extreme cases.
- Anemia may occur, often due to associated iron deficiency or recurrent infections.
Rickets Prevention
- Adequate exposure to sunlight
- Making sure that your child receives adequate amounts of Vitamin D, calcium, and phosphorus is the most effective method for preventing rickets.8Thacher, T. D., Fischer, P. R., Strand, M. A., & Pettifor, J. M. (2006). Nutritional rickets around the world: Causes and future directions. Annals of Tropical Paediatrics, 26(1), 1–16. https://doi.org/10.1179/146532806×90556 One must take foods that are rich in vitamin D, phosphorus, and calcium to prevent rickets. Such foods include fatty fish, eggs, milk, cheese, and yogurt.
- The patient takes vitamin D orally in accordance with requirements. Daily 400 IU is the dose of Vitamin D.9Shaw, N. J. (2016). Prevention and treatment of nutritional rickets. The Journal of steroid biochemistry and molecular biology, 164, 145-147.
- Breastfed infants, especially those whose mothers have limited sunlight exposure, should receive 400 IU of vitamin D daily.
- Mothers who are breastfeeding and expecting should take vitamin D.
Prognosis of Rickets
The majority of children with vitamin D deficiency due to diet respond very well to therapy. However, radiologic healing takes place within a few months. Additionally, the results from laboratory tests should also quickly return to normal. Moreover, while many bone malformations drastically improve, severely ill children may have lifelong deformities.
Conclusion
Rickets is a preventable condition that requires awareness, education, and appropriate preventative measures. It is important for parents to be vigilant in checking the symptoms of rickets and consult a doctor if any of these symptoms are present in the child. Early diagnosis and treatment can prevent long-term complications and ensure that the child’s bones develop properly. By taking a proactive approach to preventing rickets, we can help ensure that children have healthy and strong bones for a lifetime.
Refrences
- 1Gentile, C., & Chiarelli, F. (2021). Rickets in children: An update. Biomedicines, 9(7), 738.https://doi.org/10.3390/biomedicines9070738
- 2A, B. A., Dahash, & Sankararaman, S. (n.d.). Rickets – statpearls – NCBI bookshelf. Retrieved March 27, 2023, from https://www.ncbi.nlm.nih.gov/books/NBK562285/
- 3Chapman, T., Sugar, N., Done, S., Marasigan, J., Wambold, N., & Feldman, K. (2010). Fractures in infants and toddlers with it. Pediatric radiology, 40, 1184-1189.
- 4Sahay M, Sahay R. Rickets-vitamin D deficiency and dependency. Indian J Endocrinol Metab. 2012 Mar;16(2):164-76. doi: 10.4103/2230-8210.93732. PMID: 22470851; PMCID: PMC3313732.
- 5Lambert AS, Linglart A. Hypocalcaemic and hypophosphatemic rickets. Best Pract Res Clin Endocrinol Metab. 2018 Aug;32(4):455-476. doi: 10.1016/j.beem.2018.05.009. Epub 2018 Jul 4. PMID: 30086869.
- 6STONE, J. S. DEFORMITIES OF THE CHEST IN RICKETS. Transactions of the American Orthopedic Association s1-11(1):p 337-346, May 1898.
- 7Biasucci, G., Donini, V., & Cannalire, G. (2024). Rickets Types and Treatment with Vitamin D and Analogues. Nutrients, 16(3), 416. https://doi.org/10.3390/nu16030416
- 8Thacher, T. D., Fischer, P. R., Strand, M. A., & Pettifor, J. M. (2006). Nutritional rickets around the world: Causes and future directions. Annals of Tropical Paediatrics, 26(1), 1–16. https://doi.org/10.1179/146532806×90556
- 9Shaw, N. J. (2016). Prevention and treatment of nutritional rickets. The Journal of steroid biochemistry and molecular biology, 164, 145-147.



