
Biliary Dyskinesia is a disorder of the gallbladder that affects its motility, impairing its ability to effectively pass bile through the bile ducts into the small intestine. As a result, bile accumulates in the gallbladder, leading to symptoms such as pain, nausea, and vomiting. The condition also involves dysfunction of the sphincter of Oddi, a muscle at the junction of the bile and pancreatic ducts that controls bile flow. When the sphincter of Oddi is affected, bile flow out of the gallbladder is obstructed, further contributing to symptoms.1Toouli J. Biliary Dyskinesia. Curr Treat Options Gastroenterol. 2002 Aug;5(4):285-291. doi: 10.1007/s11938-002-0051-9. PMID: 12095476.
Background of Biliary Dyskinesia
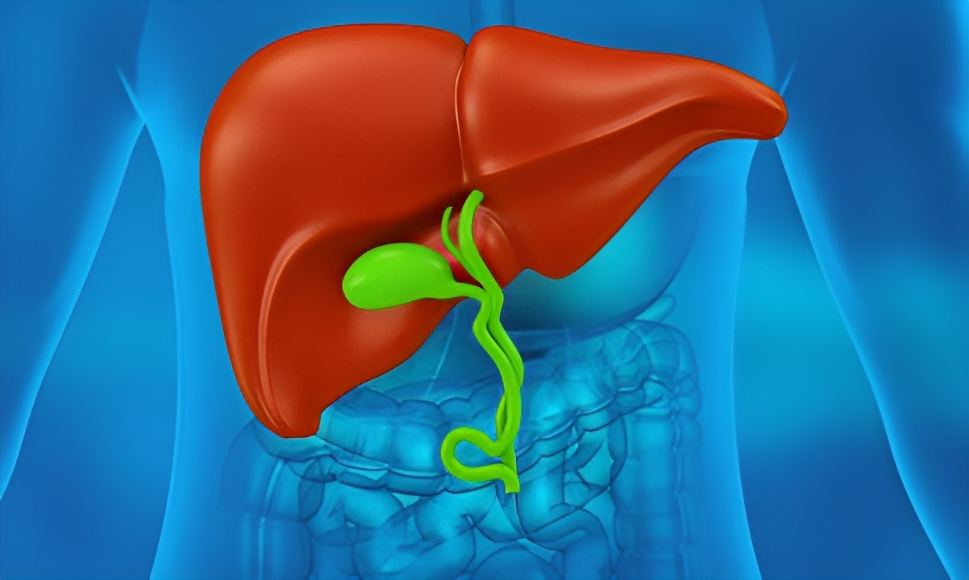
Your liver forms bile, which is yellow-green in color and liquid in consistency. The liver passes the bile into the gallbladder, where the bile is stored. The gallbladder is part of the digestive system. It is a small, pear-shaped organ on the right side of the body, under the right lobe of the liver. When you eat food, the gallbladder contracts and passes the bile into the small intestine, helping in the digestion of fats present in the food. It also helps in clearing the waste products from your body. However, in cases of biliary dyskinesia, bile remains trapped in the gallbladder, disrupting fat digestion and preventing effective waste removal. Accumulation of bile also causes the distension of the gallbladder, leading to inflammation or infections.
Causes of Biliary Dyskinesia
There is no exact cause of biliary dyskinesia. However, it may involve any damage to the nerve that supplies the biliary system, leading to the motility disorders of the gallbladder. Gastrointestinal motility disorders like esophageal dysmotility or gastroparesis also cause biliary dyskinesia. Moreover, any problem in the signaling pathway that sends signals to the gallbladder to release bile into the intestine also causes biliary dyskinesia.
Cholecystitis (Inflammation of the gallbladder) due to the presence of stones in the bile ducts also causes bile to accumulate, and in most cases, cholecystitis is associated with biliary dyskinesia. Management of cholecystitis also helps in improving the symptoms of biliary dyskinesia.2Lugo-Vicente HL. Gallbladder dyskinesia in children. JSLS. 1997 Jan-Mar;1(1):61-4. PMID: 9876649; PMCID: PMC3015221.
Risk Factors Associated with Biliary Dyskinesia:
The following factors can increase your chances of developing the condition:
Old Age:
With age, the motility of several organs decreases. Therefore, the motility of the gallbladder also decreases, and it cannot pass bile into the small intestine, leading to biliary dyskinesia.
Sex:
Females are more prone to have biliary dyskinesia. It is probably because of the sex hormone estrogen. Estrogen increases the cholesterol content of bile, causing it to crystallize. Eventually, the bile cannot flow easily from your gallbladder into your small intestine.
Obesity:
Obesity increases the body’s overall fat content and decreases the efficiency of its organs, including the gallbladder. It also increases the risk of gallstones, which accumulate bile in the gallbladder.
Stress:
Stress and anxiety increase the chance of developing biliary dyskinesia in females. Stress and anxiety cause hypokinesia (less movement), which leads to decreased motility in the body, including the gastrointestinal system and the gallbladder. This hypokinesia in the gallbladder eventually causes biliary dyskinesia.
Gastrointestinal Diseases:
If you are already suffering from any gastrointestinal disease, such as gastroparesis or esophageal dysmotility, you are at higher risk of having biliary dyskinesia. This is because motility disorders of the gastrointestinal system also affect the motility of the biliary system.
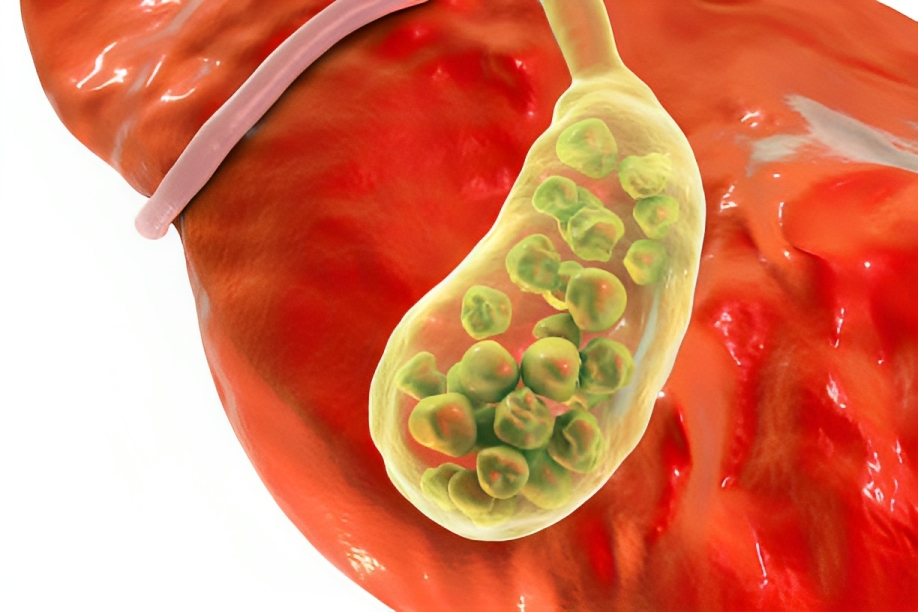
Gallstones:
Gallstones are the most common cause of cholecystitis (gallbladder inflammation). Stones obstruct bile flow into the small intestine, and the bile starts collecting in the gallbladder, causing biliary dyskinesia.3Sodeman, W. A. (2005). Functional gastrointestinal disease. In Elsevier eBooks (pp. 146–147). https://doi.org/10.1016/b978-141600203-1.50065-2
Symptoms of Biliary Dyskinesia
It presents with symptoms that resemble the symptoms of gallstones. When a large amount of bile is collected in the gallbladder, symptoms start appearing, causing infection and inflammation.4Goncalves RM, Harris JA, Rivera DE. Biliary dyskinesia: natural history and surgical results. Am Surg. 1998 Jun;64(6):493-7; discussion 497-8. PMID: 9619167.
You may feel the following symptoms:
- Severe episodic pain in the right upper quadrant of your abdomen
- Nausea
- Vomiting
- Intolerance to fatty foods
- Anorexia (Lack of appetite)
- Severe epigastric pain that occurs after eating especially fatty foods
- Bloating

What Complications can occur?
It becomes complicated when a large amount of bile accumulates in the gallbladder. Some of the complications are:
Inflammation & Infection of the Gallbladder:
It can lead to gallbladder inflammation, which is caused by the excessive accumulation of bile. This inflammation causes an infection of the gallbladder called cholecystitis. Cholecystitis can cause pain similar to the pain of biliary dyskinesia, and Cholecystectomy (removal of the gallbladder) is performed to treat it.
Indigestion of Fatty Foods:
Bile digests fat from the diet. When bile can not enter the small intestine due to this condition, fat digestion is not done correctly, leading to indigestion and bloating.
Anxiety:
It takes almost three months to diagnose the symptoms properly. You feel pain, nausea, and vomiting in these three months, and this constant state of illness leads to anxiety and depression.
Irritable Bowel Syndrome:
This condition causes improper digestion of your food. This improper digestion can cause IBS, in which you either suffer from diarrhea or constipation along with abdominal pain.5Chemmanur, A. T., MD. (n.d.). Biliary disease: background, pathophysiology, etiology. https://emedicine.medscape.com/article/171386-overview?form=fpf
How to Diagnose Biliary Dyskinesia?
It is diagnosed by taking a proper history and doing several investigations to rule out other causes of the symptoms.
Medical & Surgical History:
Your doctor may ask questions about your past medical and surgical history to make a proper diagnosis. He may also inquire about your medical history with questions such as whether you have experienced any gastrointestinal diseases, abdominal or epigastric pain, or if you have a history of gallstones or stones in other organs. They may also ask if you have undergone any surgeries, particularly those related to the gastrointestinal system.
Examination & History of the Symptoms:
It is essential that your doctor properly examine the nature of your symptoms to make a definite diagnosis. An abdominal examination is necessary to confirm the origin of the pain and to confirm that it is actually due to a problem with the gallbladder.
Moreover, it is crucial to take a detailed history related to the nature of symptoms because the pain is specific and intermittent (occurs in episodes)
Common questions your doctor may ask you:
- Do you feel more pain after eating fatty foods?
- Is the pain episodic?
- What is the intensity of your pain?
- Does vomiting relieve your pain?
These questions are essential to rule out the symptoms of other gastrointestinal tract diseases.
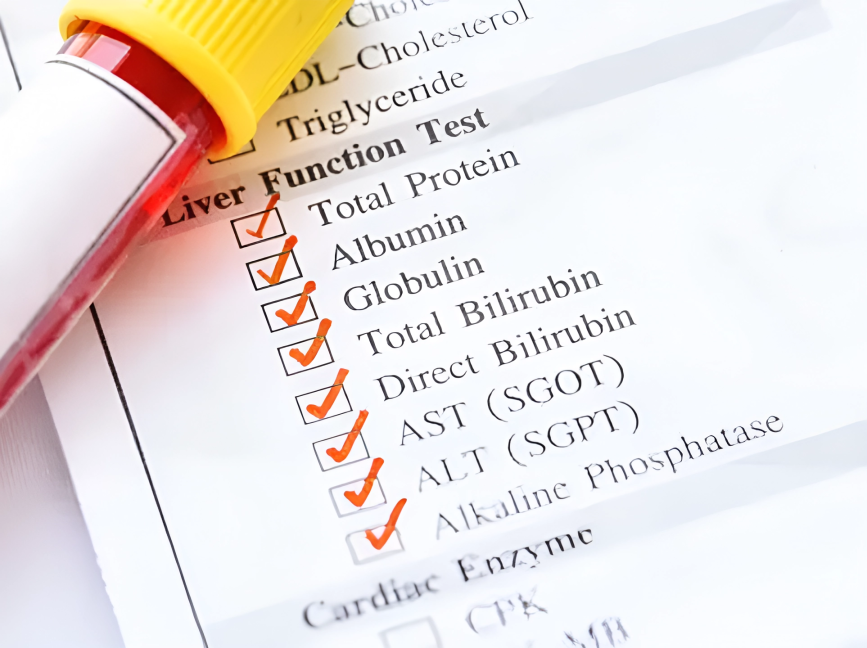
Blood Tests:
Blood tests help to see the levels of specific enzymes and substances related to the gallbladder. Your doctor can also check other enzymes related to the pancreas and liver to confirm the extent of the disease. These include:
- Bilirubin
- Liver function tests, including ALP, AST GGT, and ALT
- Pancreatic enzymes like lipases and esterases
An increase in enzyme levels indicates that the specific organ is not functioning correctly, and you need to take it seriously.
Cholecystokinin Test:
The Cholecystokinin Test, also known as the CCK stimulation test, is a diagnostic procedure used to evaluate gallbladder motility. In this test, synthetic cholecystokinin, a hormone that stimulates gallbladder contraction and bile release, is administered intravenously. The patient’s gallbladder activity is then monitored using imaging techniques such as ultrasound or cholescintigraphy.
During the test, if the patient experiences pain or discomfort following the injection, it suggests that the gallbladder is responding appropriately by contracting and releasing bile. This response helps rule out gallbladder dysfunction as a cause of the patient’s symptoms, indicating a normal gallbladder function.
However, if the patient does not experience pain or discomfort despite administering cholecystokinin, it may suggest impaired gallbladder motility, a characteristic feature of biliary dyskinesia. Along with clinical symptoms and other diagnostic tests, the Cholecystokinin Test aids in confirming the diagnosis of biliary dyskinesia and guiding appropriate treatment.6Jones MC, Vaqar S. Cholecystokinin Test. 2023 Jan 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 32809658.
HIDA Scan:
A hepatobiliary iminodiacetic acid scan (HIDA scan) diagnoses several problems in your liver and gallbladder. In this scan, a radiologist injects a tracer into your body through a vein. This tracer flows from your liver into the gallbladder along with the bile. From the gallbladder, it enters into your small intestine. A camera records the flow of the tracer. This procedure diagnoses abnormalities like stones or adhesions in your gallbladder, liver, or small intestine.
Moreover, a HIDA scan helps calculate the gallbladder ejection fraction, the amount of bile that flows outside the gallbladder. You likely have biliary dyskinesia if the ejection fraction is less than 40%.
Ultrasound:
In many patients, this condition presents with gallstones. Therefore, if there is suspicion of gallstones, it is better to have an abdominal ultrasound. However, a doctor cannot detect biliary dyskinesia alone on the ultrasound.
Endoscopy:
In rare cases, an endoscope helps diagnose this condition. Your doctor inserts an endoscope through your mouth into the small intestine. An endoscope also helps analyze whether Oddi’s sphincter is working correctly.
Manometry:
Manometry helps to find out the cause of biliary dyskinesia. In some cases, the stenosis of the sphincter of Oddi causes biliary dyskinesia. Manometry helps in diagnosing the stenosis of the sphincter.7Ham JM, Bolin TD, Wilton N, Stevenson D, Jefferies S. The diagnosis and treatment of functional disorders of the biliary tract. Aust N Z J Surg. 1978 Oct;48(5):494-9. doi: 10.1111/j.1445-2197.1978.tb00029.x. PMID: 285695.
How to Treat Biliary Dyskinesia?
Biliary Dyskinesia can be managed through various treatment approaches tailored to the individual’s symptoms and specific condition. Treatment options may include:
Painkillers:
The pain of this condition is severe in intensity. You can use painkillers like paracetamol to decrease the intensity of pain.
Antiemetics:
If you are feeling nauseous along with the pain, your doctor may prescribe antiemetics like ondansetron or prochlorperazine.
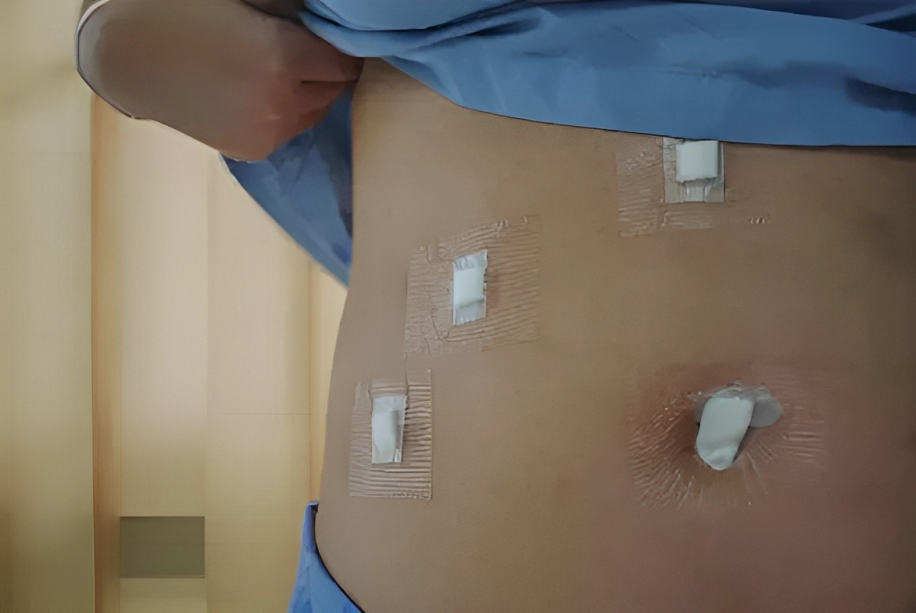
Cholecystectomy:
The only definite treatment for this condition is Cholecystectomy, which is the removal of your gallbladder. Cholecystectomy can be done either by laparoscopy or by open surgery. Laparoscopic Cholecystectomy is a far better option than open surgery to remove your gallbladder because it is minimally invasive, with fewer scars and fewer complications.
Sphincterotomy:
The stenosis of the sphincter of Oddi causes bile to collect in the gallbladder, causing biliary dyskinesia. In this case, sphincterotomy is performed. Most of the patients recover from biliary dyskinesia through this procedure.8Thosani, A. J., MD. (n.d.). Acalculous Cholecystopathy: Overview, presentation, Differential Diagnosis. https://emedicine.medscape.com/article/172013-overview#?form=fpf
What to expect after Cholecystectomy?
When your gallbladder is removed by laparoscopic Cholecystectomy, you can go home on the same day, as it is a minimally invasive procedure. When your gallbladder is removed, your liver sends bile directly into your small intestine. It takes a few weeks for your body to adjust without the gallbladder. Your doctor may advise avoiding oily or fatty foods for a few months. It would help if you took a healthy diet to prevent vomiting or gas.
Dietary Modifications for Biliary Dyskinesia
If you have biliary dyskinesia, you should eat food that is low in fat because your gallbladder cannot digest fat properly. Eat a healthy diet of fruits, vegetables, and nuts. Use beneficial and essential oils and avoid fast foods as much as possible.
If you have undergone Cholecystectomy due to biliary dyskinesia, you should eat a low-fat diet as long as your doctor advises you to.
Prognosis
Biliary dyskinesia is not severe, so its prognosis is quite good. 90% of the patients recover after Cholecystectomy (removal of the gallbladder). The prediction of biliary dyskinesia is also good after sphincterotomy if the problems lie in the sphincter of Oddi. However, eating a low-fat diet would be best to recover from the disease completely.9Geiger TM, Awad ZT, Burgard M, Singh A, Davis W, Thaler K, Miedema BW. Prognostic indicators of quality of life after Cholecystectomy for biliary dyskinesia. Am Surg. 2008 May;74(5):400-4. PMID: 18481495.
Difference between Biliary Dyskinesia & Gastroparesis
Biliary dyskinesia and gastroparesis have the exact mechanism but involve different organs. In gastroparesis, your stomach is affected, while the gallbladder is affected in biliary dyskinesia.
In gastroparesis, the nerves and muscles of the stomach become weak. Therefore, your stomach cannot easily pass the food into your small intestine. In that way, food remains in your stomach for a long time, leading to bloating, acidity, and gas. On the other hand, in biliary dyskinesia, nerves of the gallbladder cannot function properly, causing the bile to accumulate in it for an extended period.
Conclusion
In conclusion, biliary dyskinesia affects the motility of the gallbladder, which is either due to the dysfunction of the sphincter of Oddi or decreased activity of the nerves supplying the gallbladder. It is a treatable disease, and it is only treated by removing your gallbladder. Eating a healthy diet after Cholecystectomy would be best because you cannot digest the fat properly without the gallbladder.
After Cholecystectomy, you can recover in two or three days with proper rest and a healthy diet.
Refrences
- 1Toouli J. Biliary Dyskinesia. Curr Treat Options Gastroenterol. 2002 Aug;5(4):285-291. doi: 10.1007/s11938-002-0051-9. PMID: 12095476.
- 2Lugo-Vicente HL. Gallbladder dyskinesia in children. JSLS. 1997 Jan-Mar;1(1):61-4. PMID: 9876649; PMCID: PMC3015221.
- 3Sodeman, W. A. (2005). Functional gastrointestinal disease. In Elsevier eBooks (pp. 146–147). https://doi.org/10.1016/b978-141600203-1.50065-2
- 4Goncalves RM, Harris JA, Rivera DE. Biliary dyskinesia: natural history and surgical results. Am Surg. 1998 Jun;64(6):493-7; discussion 497-8. PMID: 9619167.
- 5Chemmanur, A. T., MD. (n.d.). Biliary disease: background, pathophysiology, etiology. https://emedicine.medscape.com/article/171386-overview?form=fpf
- 6Jones MC, Vaqar S. Cholecystokinin Test. 2023 Jan 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 32809658.
- 7Ham JM, Bolin TD, Wilton N, Stevenson D, Jefferies S. The diagnosis and treatment of functional disorders of the biliary tract. Aust N Z J Surg. 1978 Oct;48(5):494-9. doi: 10.1111/j.1445-2197.1978.tb00029.x. PMID: 285695.
- 8Thosani, A. J., MD. (n.d.). Acalculous Cholecystopathy: Overview, presentation, Differential Diagnosis. https://emedicine.medscape.com/article/172013-overview#?form=fpf
- 9Geiger TM, Awad ZT, Burgard M, Singh A, Davis W, Thaler K, Miedema BW. Prognostic indicators of quality of life after Cholecystectomy for biliary dyskinesia. Am Surg. 2008 May;74(5):400-4. PMID: 18481495.



