
Biliary sludge, also called gallbladder sludge, forms when bile remains in the gallbladder for an extended period and thickens into a mixture of cholesterol crystals, calcium bilirubinate granules, mucin, and other debris.1Jungst D, et al. “Gallbladder sludge and stones: Pathogenesis and natural history.” Digestive Diseases, 2000. While not a disease on its own, biliary sludge often represents an early stage of gallbladder dysfunction and may progress to gallstones or gallbladder inflammation (cholecystitis) if left unaddressed.2Portincasa P, et al. “Cholecystitis and biliary sludge: Clinical overview.” Best Practice & Research Clinical Gastroenterology, 2006.
The gallbladder is a small organ below the liver on the upper right side of your abdomen. It stores bile, a greenish-yellow fluid produced by the liver, which is released into the small intestine after meals to help digest fats.

Sludge tends to form when the gallbladder doesn’t empty properly. In such cases, the bile becomes concentrated and its components—especially cholesterol and calcium salts—begin to precipitate.3Shaffer EA. “Epidemiology and risk factors for gallstone disease.” Best Practice & Research Clinical Gastroenterology, 2006.
What Is Biliary Sludge?
Under certain conditions, the normally fluid bile can become thickened, forming a sludge-like substance.4Lee SP. “Pathogenesis of gallstones and biliary sludge.” Hepatology, 1990.
Biliary sludge isn’t a solid stone, but it’s thicker than bile and can block bile ducts, causing symptoms and complications. This condition can be silent, remaining undetected and symptom-free for long periods. In fact, biliary sludge is often found incidentally on ultrasound imaging done for unrelated reasons.5Stinton LM, Shaffer EA. “Epidemiology of gallbladder disease.” Gastroenterology Clinics of North America, 2010. However, in some cases, it can lead to inflammation, biliary colic, or progress to gallstone disease.6Venneman NG, van Erpecum KJ. “Pathogenesis of gallstones.” Gastroenterology Clinics, 2010.
Gallbladder sludge is often diagnosed in people with gallbladder or liver problems, since they’re more likely to get tested in imaging procedures that detect such findings.
Biliary Sludge Symptoms
Several patients fail to detect gallbladder sludge, as the condition mostly does not present with noticeable symptoms7Shiffman ML. “Gallbladder sludge in the critically ill.” Gastroenterology, 2002. Outpatient imaging scans commonly uncover this condition because most of those affected are unaware they have gallbladder sludge. However, it occasionally can lead to symptoms that medical professionals mistake for gallbladder inflammation or gallstone illness.8Ko CW, Lee SP. “Epidemiology and natural history of gallstone disease.” Gastroenterology Clinics, 2010.
The main symptom experienced by most patients involves stomach pain immediately after eating a meal in the area under the ribs and on top of the right quadrant. Individuals who have gallbladder sludge often develop nausea or vomiting along with a sense of being full and bloating. The pain spreads toward the right shoulder, back, or chest, which produces symptoms resembling other health conditions.
Additional symptoms may include:
- Pale or clay-colored stools
- Loose or fatty stools (Steatorrhea)
- Fever
- Intermittent pain that comes and goes
Symptoms that appear in some cases also vary in intensity or completely disappear at different times. Symptoms appear in approximately 10% to 15% of individuals with gallbladder sludge, while other people may progress to forming gallstones or developing an inflamed gallbladder.9Kiewiet RM, et al. “Acute biliary pancreatitis: Diagnosis and treatment.” BMJ, 2017. Acute pancreatitis emerges only in exceptional cases; often, other patients may never experience any related symptoms.
A formal diagnosis becomes important because these signs also appear in other digestive and biliary disorders before any appropriate treatment plan can be established.
What Causes Biliary Sludge?
Gallbladder sludge forms because bile remains in the gallbladder for a long time, mostly when bile flow is delayed or impaired.10Di Ciaula A, et al. “Bile composition in health and disease.” Gut and Liver, 2017.
Lifestyle and Medical Triggers
In certain situations, the formation of sludge is increased, such as pregnancy, especially when accompanied by dietary restrictions or rapid hormonal changes. Although it occurs rarely, it seems to develop more often among individuals who have particular health situations or lifestyle behaviors
Groups at higher risk include:
- Females have a higher prevalence of gallbladder issues.
- Individuals with Native American or Mexican American ancestry.
- People receiving nutrition intravenously (parenteral nutrition).
- Those recovering from organ transplants.
- Patients with critical illnesses.
- Individuals with diabetes or insulin resistance.
- People who had obesity along with rapid weight loss.
Health-Related Risks
Gallbladder sludge is also formed under some health conditions. These include:
- Cirrhosis, which impairs liver function.
- Crohn’s disease and other gastrointestinal disorders affect nutrient absorption.
- Hemolytic anemia results in excess bilirubin production.
- Individuals who have increased blood pressure, blood sugar, cholesterol levels, and obesity.
- Infections of the bile ducts
- Low HDL (good) cholesterol
- Elevated triglyceride levels
Along with these medical conditions, certain medications, the use of alcohol, and major surgeries or illnesses can raise the risk as well.
Genetic Factors
Genetics possibly contributes to the development of gallstones. The LITH (lithogenic) gene variations affect how the body processes cholesterol and bile acids.11Buch S, et al. “A genome-wide association scan identifies the hepatic cholesterol transporter ABCG8 as a susceptibility gene for symptomatic gallstone disease.” Nature Genetics, 2007. These variations increase a person’s chance of developing symptomatic gallstones and gallbladder disease. About 30% of people who experience gallstone symptoms possess at least one of these genetic variants.
Biliary Sludge vs. Gallstones: What’s the Difference?
It’s easy to confuse these two, but they’re not identical.
| Feature | Biliary Sludge | Gallstones |
|---|---|---|
| Consistency | Semi-solid mixture of crystals and mucus | Solid stone-like deposits |
| Size | Microscopic or sludge-like | Can range from sand-grain to golf ball size |
| Symptoms | Often asymptomatic, can mimic gallstones | Similar, but usually more severe and persistent |
| Detection | Seen on ultrasound as echogenic bile | Seen as distinct stones on imaging |
| Potential to resolve | It may go away on its own | Typically requires treatment if symptomatic |
Sludge can be the precursor to gallstones, or it may disappear entirely once the underlying issue resolves.12Lammert F, et al. “Genetics and pathogenesis of gallstones.” Seminars in Liver Disease, 2008.
How Is Biliary Sludge Diagnosed?
Anyone who feels unexplained abdominal pain, especially in the upper right side, should seek medical attention. Repeated intense pain requires medical examination for possible severe conditions, including pancreatitis, together with pancreatic cancer.
Initial Evaluation
Your provider will begin with a thorough symptom history and a physical exam to assess abdominal tenderness. Based on suspicion of gallbladder problems, diagnostic imaging is usually recommended.
Imaging Tests
The diagnostic imaging test for evaluation of gallbladder sludge should begin with a transabdominal ultrasound examination.13Erpecum KJ. “Pathogenesis of gallstones.” Neth J Med, 2003. This non-invasive test uses sound waves to visualize the gallbladder. Sludge appears as a dense material that settles at the bottom of the gallbladder.
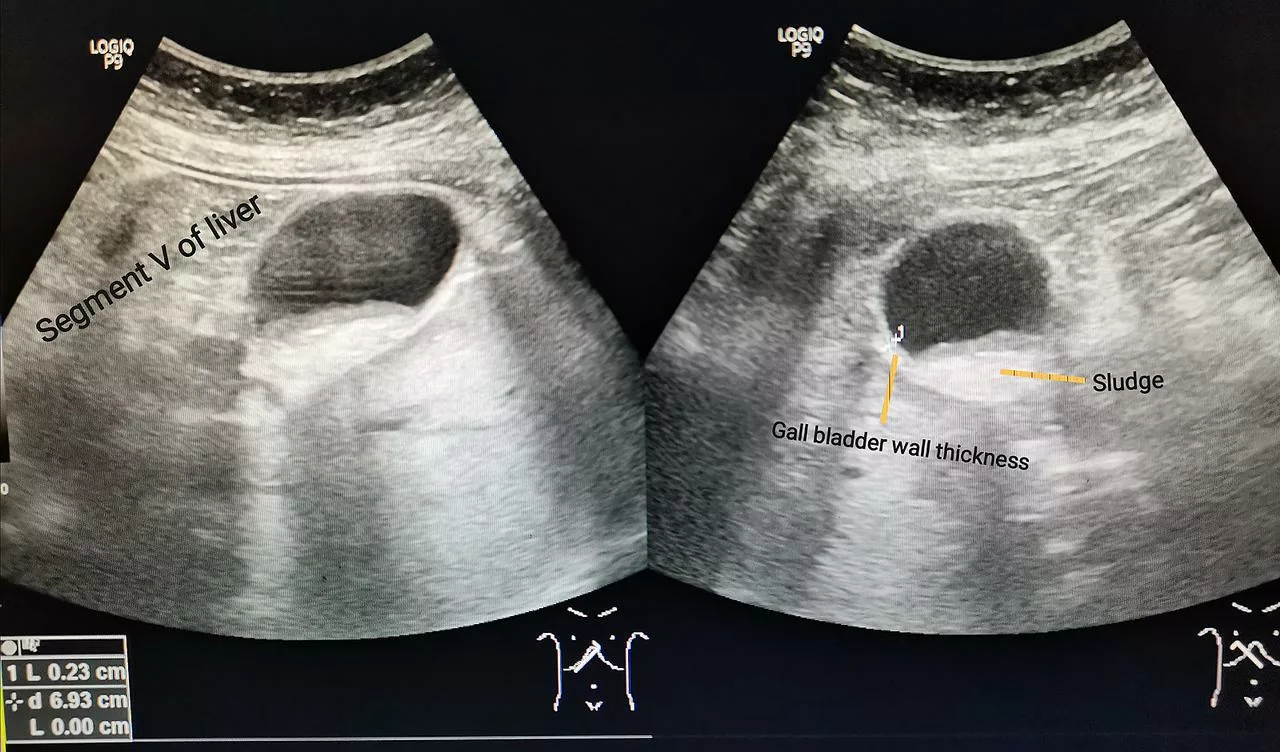
Image Credit: Cerevisae. “Ultrasound of gall bladder with sludge.” Wikimedia Commons, 11 April 2022. Licensed under CC BY-SA 4.0.
Gallbladder sludge can be found accidentally during imaging done for other abdominal issues.
Advanced Diagnostic Procedures
If the diagnosis is unclear or if complications are suspected, additional procedures may be used:
- Endoscopic Ultrasound (EUS): Combines endoscopy and ultrasound, inserting a thin, flexible tube with a small camera and ultrasound probe through the mouth into the digestive tract to closely examine the gallbladder.
- Endoscopic Retrograde Cholangiopancreatography (ERCP): An Invasive test that allows visual examination and sampling of bile.
Laboratory Tests
The physician might combine imaging tests with blood tests, which evaluate liver function while testing for signs of infection, as well as cholesterol levels, bilirubin, and electrolyte concentrations. The results from these tests show whether sludge is causing inflammation or an underlying metabolic or hepatic issue contributing to its formation.
Biliary Sludge Treatment
Treatment depends on symptoms and complications.
Watchful Monitoring for Non-Symptomatic Sludge
Sludge formation in the gallbladder usually disappears by itself when doctors happen to find it by chance, without any symptoms. Doctors often choose a “wait-and-watch” approach for observing your health condition since you do not present inflammation or pain symptoms. They commonly observe this condition because the patient experiences reversible conditions like illness and pregnancy that generate temporary sludge.14Bar Dayan Y, et al. “Natural course of biliary sludge.” Hepatology, 1993.
Medical Management
For those with recurrent symptoms or mild discomfort, medical management is a viable option. One of the main treatments involves the bile acid ursodeoxycholic acid (Actigall), which helps to dissolve the sludge and improve bile composition. However, it’s important to note that ursodeoxycholic acid is not effective for treating existing gallstones and is typically used in cases where sludge has been definitively diagnosed.15Gatta A, et al. “Ursodeoxycholic acid in the treatment of liver and biliary diseases.” Digestive and Liver Disease, 2007.
In addition to medication, lifestyle changes play a crucial role in managing biliary sludge:
- Avoiding alcohol
- Preventing rapid weight loss or gain
- Maintaining a balanced, fiber-rich diet
- Staying physically active
These approaches work together to prevent the return of gallbladder problems and support overall gallbladder function.
Dietary Adjustments for Gallbladder Health
A balanced, gallbladder-friendly diet can help prevent the accumulation of sludge and support overall gallbladder function. Key dietary recommendations include:
- Use fresh fruits in your diet along with beans, legumes, whole grains, and vegetables.
- Limit refined carbohydrates, sweet foods, and processed items.
- Select healthy fats such as olive oil, fish oil instead of over-saturated or trans fats.
- High-fat desserts, along with fried foods, should be strictly avoided.
- Moderate your sodium intake.16Grundy SM. “Cholesterol and gallstone formation.” New England Journal of Medicine, 1978.
Gradual weight loss is necessary as rapid weight reduction among overweight individuals deteriorates their risk of developing both sludge and gallstones.
Research by some studies links coffee consumption to reduced chances of specific gallbladder issues, but experts need more research to confirm this benefit.17Leitzmann MF, et al. “Coffee intake is associated with reduced risk of symptomatic gallstone disease in women.” Gastroenterology, 2002.
Surgical Treatment: Cholecystectomy
In cases where biliary sludge leads to persistent symptoms, complications, or gallstone formation, surgical intervention may be necessary. The most common procedure is cholecystectomy, the removal of the gallbladder. This is typically performed via laparoscopic surgery, a minimally invasive procedure done under general anesthesia.18Strasberg SM. “Cholecystectomy and its complications.” Surgical Clinics of North America, 1994. This procedure:
- Prevents sludge recurrence because the bile no longer collects in the gallbladder
- It is done in most cases through laparoscopy, called laparoscopic cholecystectomy, as it’s a minimally invasive method.
Most patients maintain normal health without a gallbladder because bile continues directly to the small intestine.
Is Biliary Sludge Dangerous?
While biliary sludge itself is often asymptomatic and may resolve on its own, it can lead to more serious conditions if left untreated. Possible complications include:
- Gallstone formation.
- Gallbladder inflammation (cholecystitis).
- Pancreatitis occurs when the pancreatic duct gets blocked by sludge.
- Biliary colic or obstruction.19Afdhal N. “Gallstones and biliary disease.” Harvard Medical School Publishing.
This is why even asymptomatic patients should be monitored and need close follow-up.
Is biliary sludge seen in pregnancy dangerous?
Medical professionals should observe biliary sludge, although it does not always require direct intervention. It often resolves after childbirth. However, if it causes symptoms, your OB-GYN and gastroenterologist may work together to manage it.20Bender JS, et al. “Management of biliary disease during pregnancy.” American Surgeon, 1992.
How is biliary sludge different from thick bile?
They’re very similar. Thick bile is sometimes used as a layman’s term for biliary sludge. Both refer to abnormal bile consistency21Parkman HP, et al. “Bile composition and gallbladder function.” Digestive Diseases and Sciences, 1998.
Final Thoughts
Biliary sludge may not be as well-known as gallstones, yet people should pay attention to it. It can be silent, or it can be the big reason for significant gastrointestinal symptoms.
Upper abdominal discomfort along with continuing nausea deserves professional medical evaluation, so you should not ignore these symptoms. Get it checked out. Medical treatment for the condition becomes simpler when detection happens earlier, which also decreases the risk of potential complications occurring in the future.22European Association for the Study of the Liver. “EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones.” Journal of Hepatology, 2016.
Refrences
- 1Jungst D, et al. “Gallbladder sludge and stones: Pathogenesis and natural history.” Digestive Diseases, 2000.
- 2Portincasa P, et al. “Cholecystitis and biliary sludge: Clinical overview.” Best Practice & Research Clinical Gastroenterology, 2006.
- 3Shaffer EA. “Epidemiology and risk factors for gallstone disease.” Best Practice & Research Clinical Gastroenterology, 2006.
- 4Lee SP. “Pathogenesis of gallstones and biliary sludge.” Hepatology, 1990.
- 5Stinton LM, Shaffer EA. “Epidemiology of gallbladder disease.” Gastroenterology Clinics of North America, 2010.
- 6Venneman NG, van Erpecum KJ. “Pathogenesis of gallstones.” Gastroenterology Clinics, 2010.
- 7Shiffman ML. “Gallbladder sludge in the critically ill.” Gastroenterology, 2002.
- 8Ko CW, Lee SP. “Epidemiology and natural history of gallstone disease.” Gastroenterology Clinics, 2010.
- 9
- 10Di Ciaula A, et al. “Bile composition in health and disease.” Gut and Liver, 2017.
- 11Buch S, et al. “A genome-wide association scan identifies the hepatic cholesterol transporter ABCG8 as a susceptibility gene for symptomatic gallstone disease.” Nature Genetics, 2007.
- 12Lammert F, et al. “Genetics and pathogenesis of gallstones.” Seminars in Liver Disease, 2008.
- 13Erpecum KJ. “Pathogenesis of gallstones.” Neth J Med, 2003.
- 14Bar Dayan Y, et al. “Natural course of biliary sludge.” Hepatology, 1993.
- 15Gatta A, et al. “Ursodeoxycholic acid in the treatment of liver and biliary diseases.” Digestive and Liver Disease, 2007.
- 16Grundy SM. “Cholesterol and gallstone formation.” New England Journal of Medicine, 1978.
- 17Leitzmann MF, et al. “Coffee intake is associated with reduced risk of symptomatic gallstone disease in women.” Gastroenterology, 2002.
- 18Strasberg SM. “Cholecystectomy and its complications.” Surgical Clinics of North America, 1994.
- 19Afdhal N. “Gallstones and biliary disease.” Harvard Medical School Publishing.
- 20Bender JS, et al. “Management of biliary disease during pregnancy.” American Surgeon, 1992.
- 21Parkman HP, et al. “Bile composition and gallbladder function.” Digestive Diseases and Sciences, 1998.
- 22European Association for the Study of the Liver. “EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones.” Journal of Hepatology, 2016.




{kind=link}